U.S. Birthrates Fall to a Record Low (click here to read article)
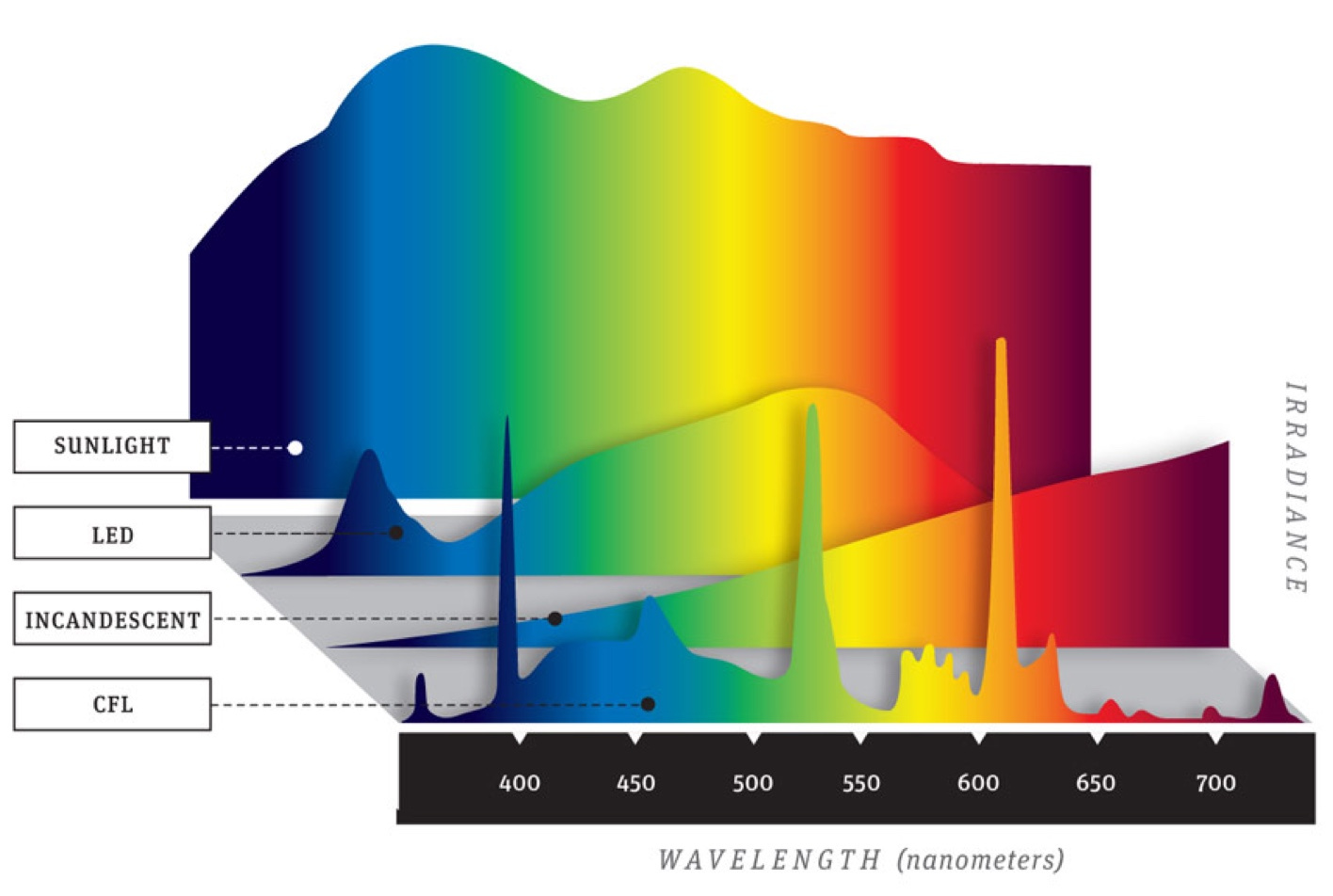
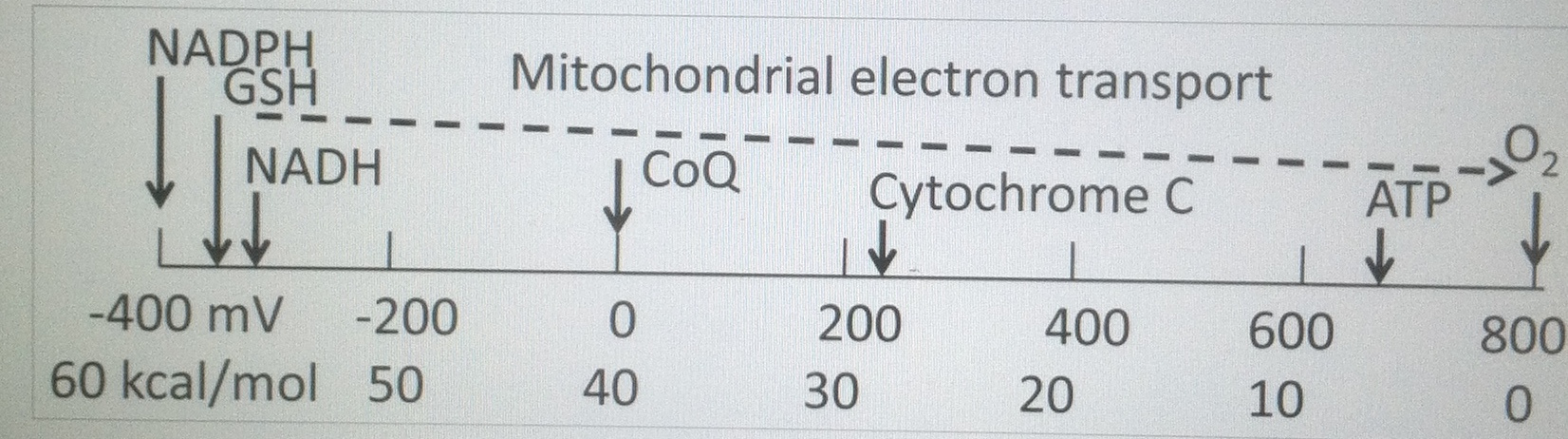
Alchemist & Metaphysician = ancestral dogmatic beliefs are that biochemistry is definitive science. Biochemistry is really a solid state story of how light alters valence electrons within hydrated semiconductive proteins. This light is capable of changing their physiologic ability as the electromagnetic signals on the surfaces of them changes geometry in their lattice. This is why electromagnetic charge changes always involve shape shifting of proteins made by DNA surrounded by water made by mitochondria. Life runs on being able to harness the energy of an excited electron to the ground state. Life cannot do this well when pseudohypoxia exists at cytochrome one with lowered NAD+. Technology’s nnEMF and blue light cause this quickest today.
The cost of a high aerobic capacity is low fertility so that we can maintain our cortisol pathways from LDL and Vitamin A as I mentioned the Hormone 101 & 102 blogs ages ago. This is why the pregnenolone steal syndrome exists. Cortisol over sex steroids is due to the use of oxygen as the terminal electron acceptor in human mitochondria. So when cortisol drops chronically this tells you that your environment is not allowing you to effectively utilize oxygen in your mitochondria as a terminal electron acceptor. What does that mean in english? It means your ubiquitination levels are raised and your mitochondria are pseudohypoxic. This means you are using other gases to perform the tasks that oxygen used to when your environment was more optimized.
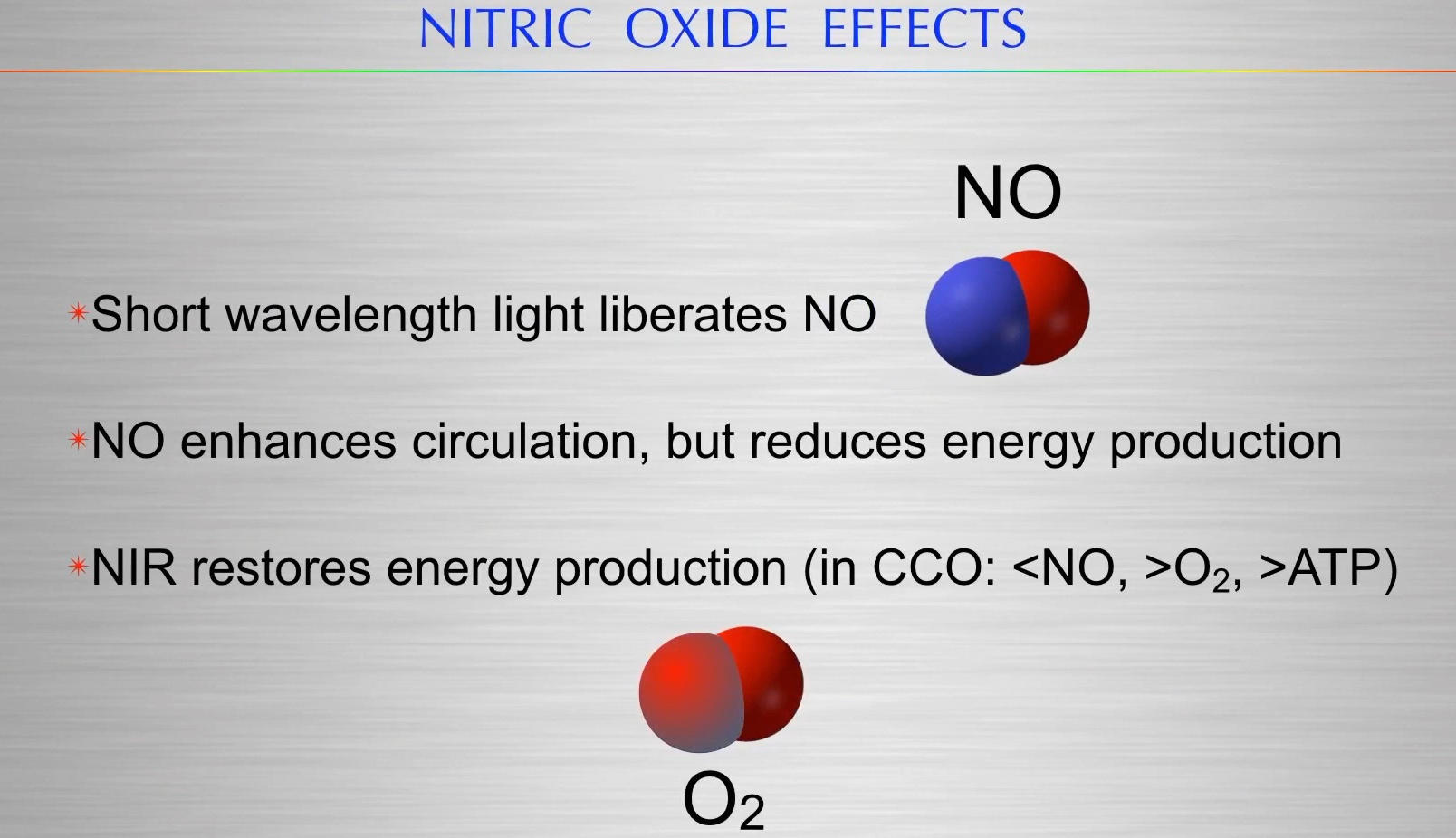
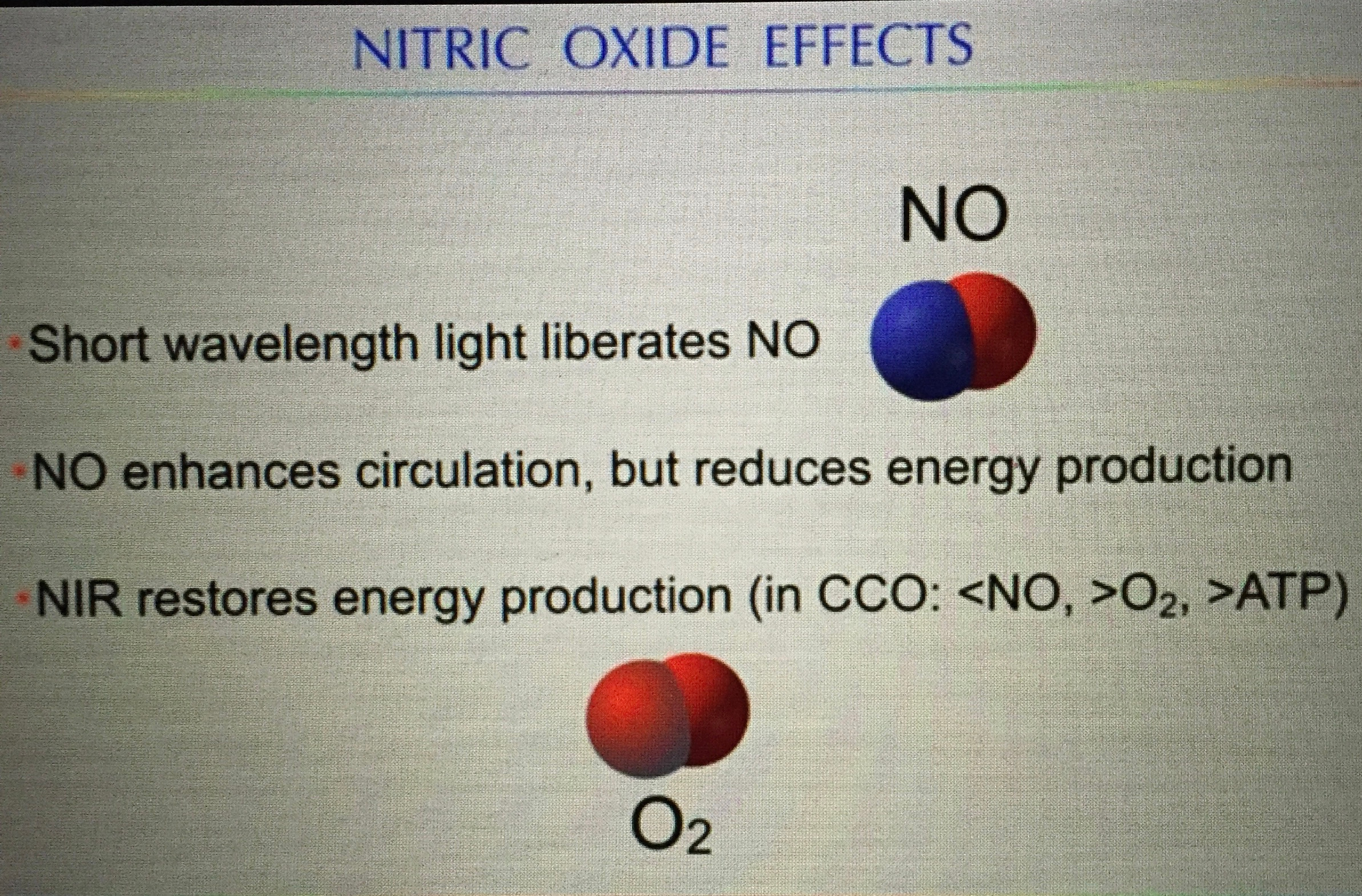
This causes us to use too much NO, H2S, and CO. These are sub-optimal choices and this leads to altered cortisol and overall hormone panels. All these changes lead to a lack of catalase in cells and altered UV light light release in cells (too much) and all these sequential changes fuel this low fertility and a low cortisol. When you begin to read all the details of the ubiquitin series you will see how pseudohypoxia plays into every mechanism of disease we have in biology and medicine and then you will see this is the huge problem our environment creates and it alters the optical non linear communication pathways between the mitochondria and nucleus.
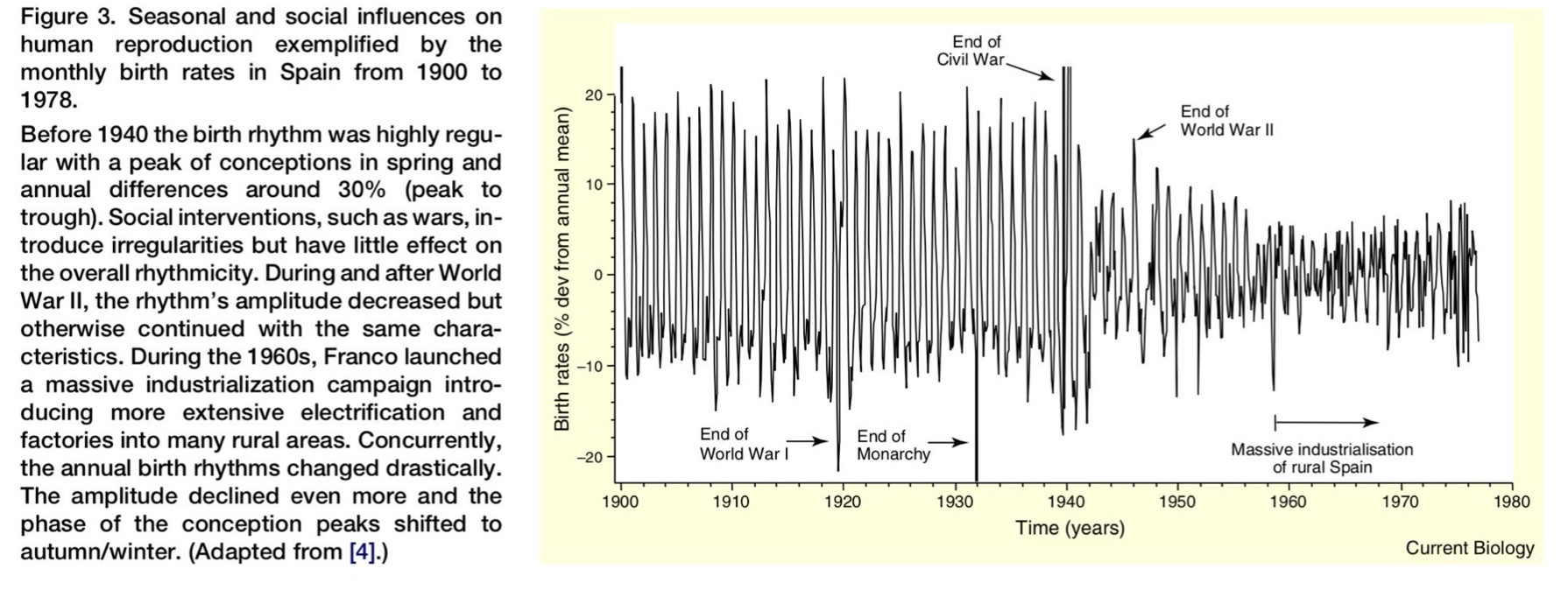
The effect of tech on fertility is linked to the NAD+ ration to NADH. Pseudohypoxia creates infertility. American births down to their smallest total in 35 years: “The general fertility rate fell 2% to 58.2 births per 1,000 women aged 15 to 44, its lowest level since the government began tracking the figure in 1909. Pseudohypoxia= leptin resistance = infertility = extinction is a synonym for infertility.
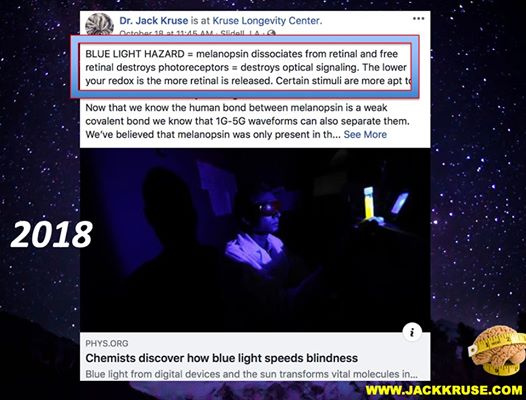
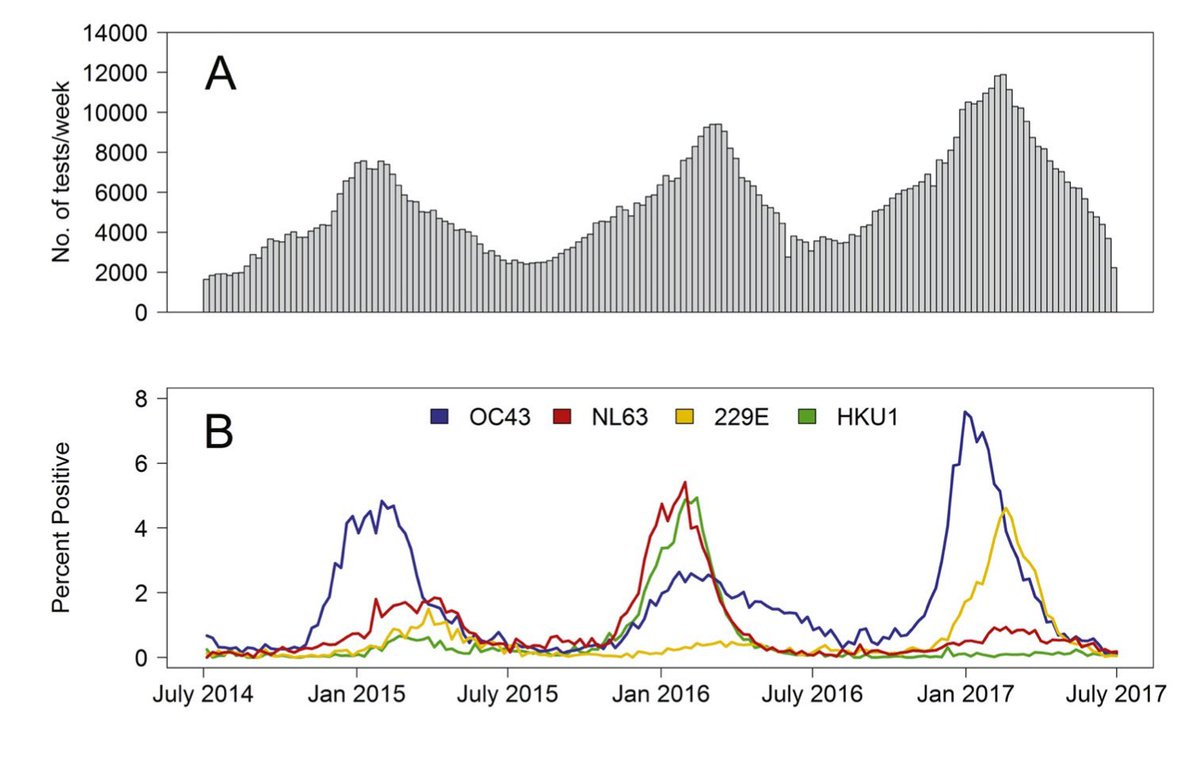
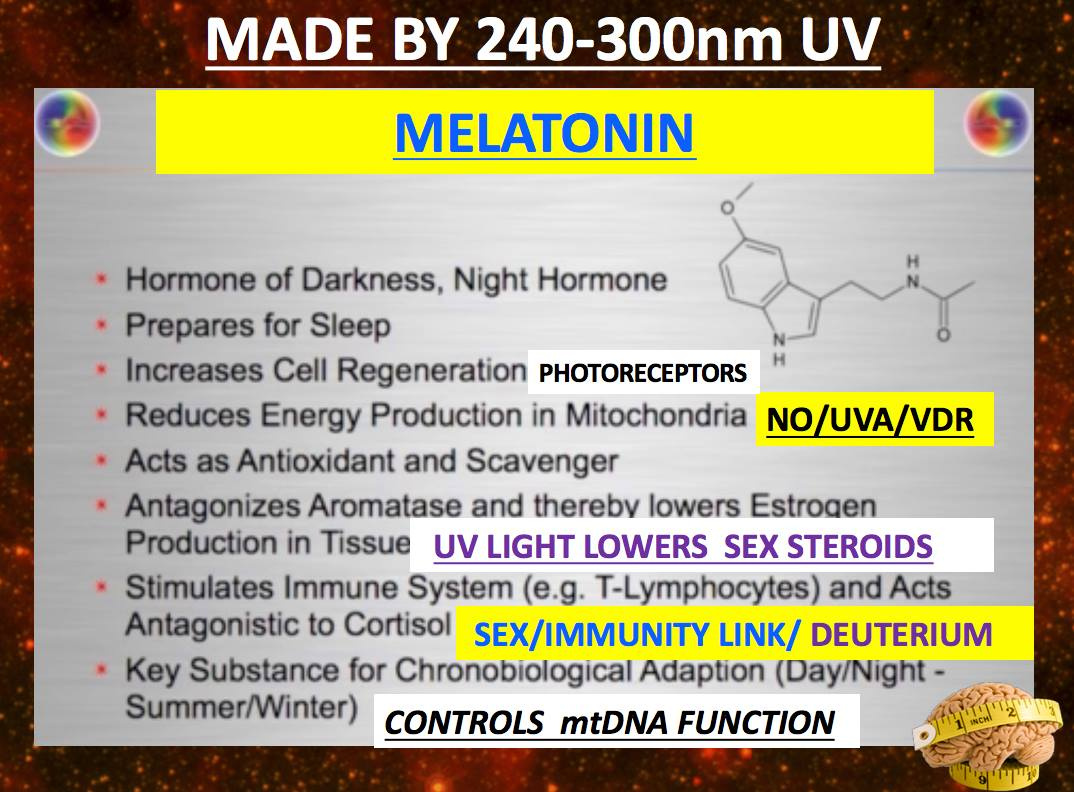
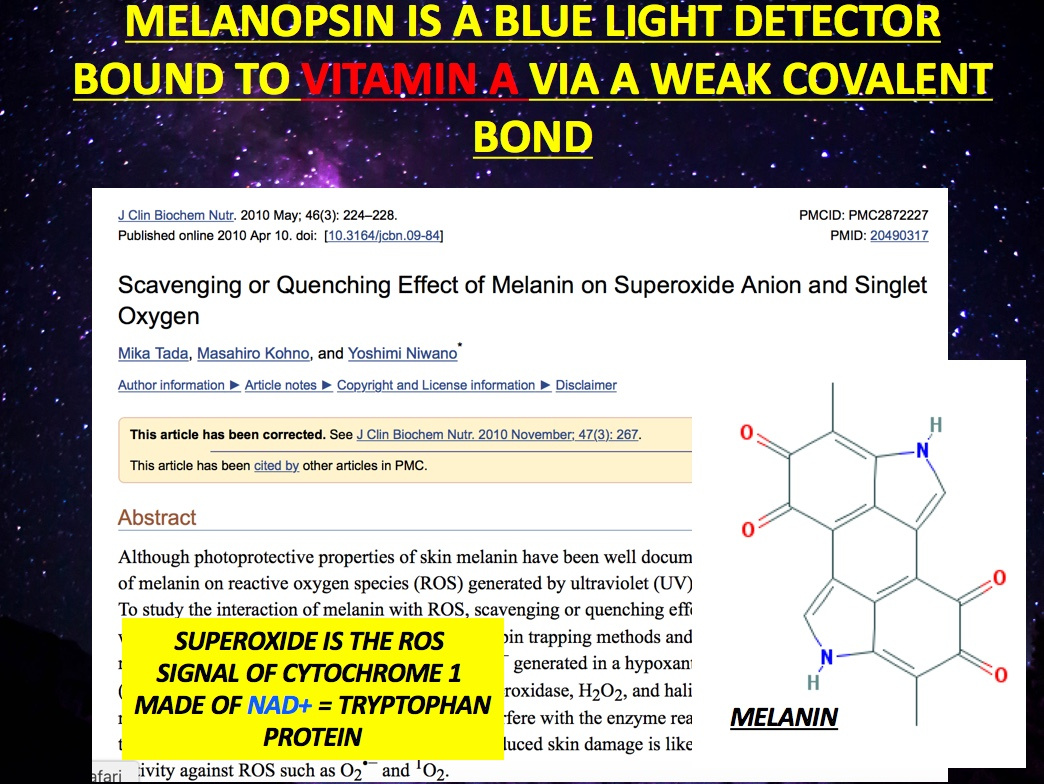
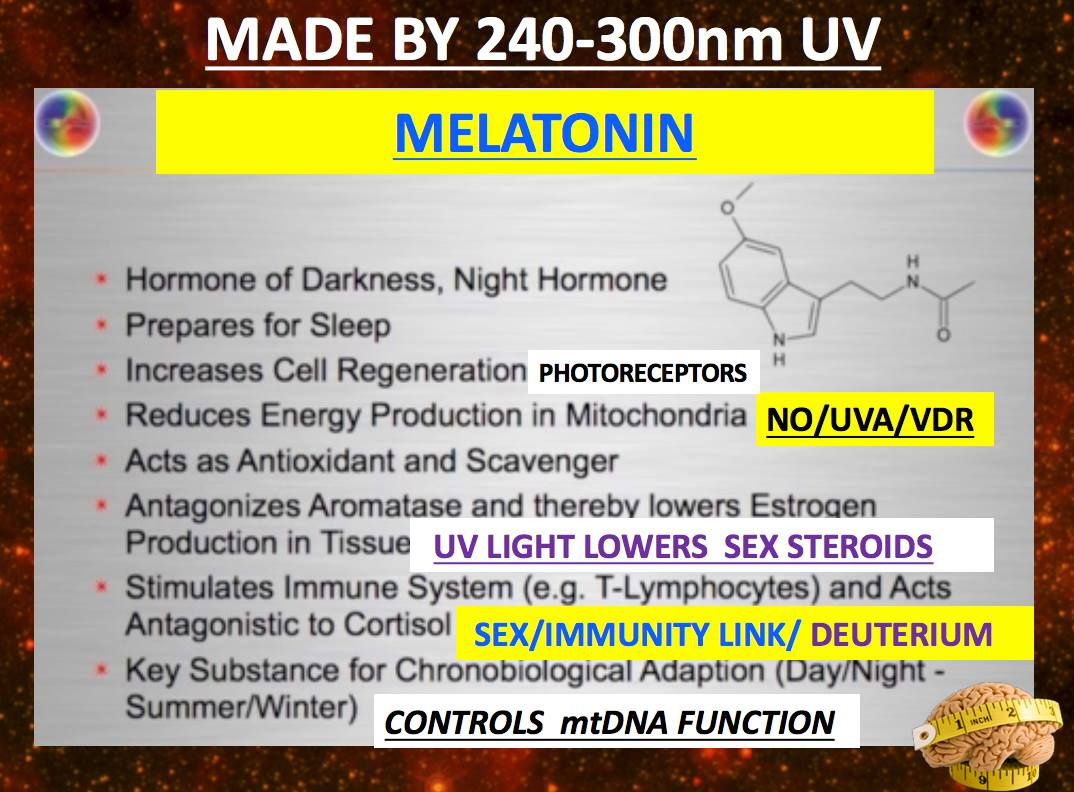
Is fecundity, fertility, and successful pregnancy all linked to circadian biology via melatonin control over apoptosis and autophagy in mitochondria? The answer appears to be a big YES. This has huge implications for extinction levels of events in anything that alters melatonin levels. It is now clear melanopsin function does this with blue light and nnEMF. I wonder how long it will take the non-Black Swans out there to get this rather simple, yet significant message?
Melatonin also appears to play an important role in modulating the immune system so a fertilized egg can be implanted. A fertilized egg has different DNA and cell markings than our own cells. In most cases, our tissues would recognize this forming embryo as an invader and the immune system would attack. Instead, our bodies welcome the rapidly dividing ball of cells as a welcome guest. What causes this unusual reaction?
Researchers are not sure exactly how this immune modulation happens but melatonin appears to play a crucial role. Melatonin is made by the placenta and appears to protect newly implanted pregnancies from immune attack while encouraging the growth of blood vessels and other changes needed to sustain a healthy pregnancy. In addition, melatonin made by the placenta is transferred to the fetus and may play an important role in the child’s prenatal development.
SUMMARY:
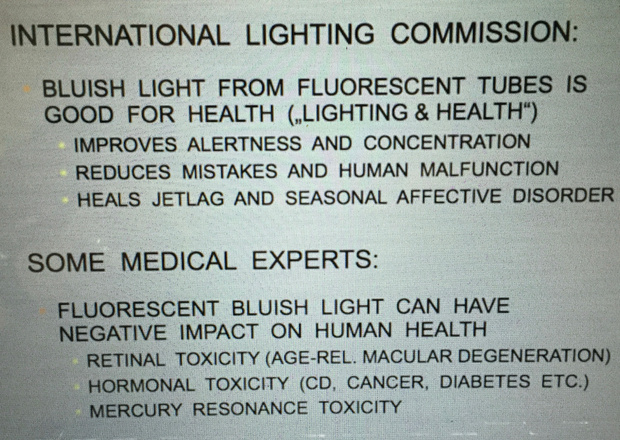
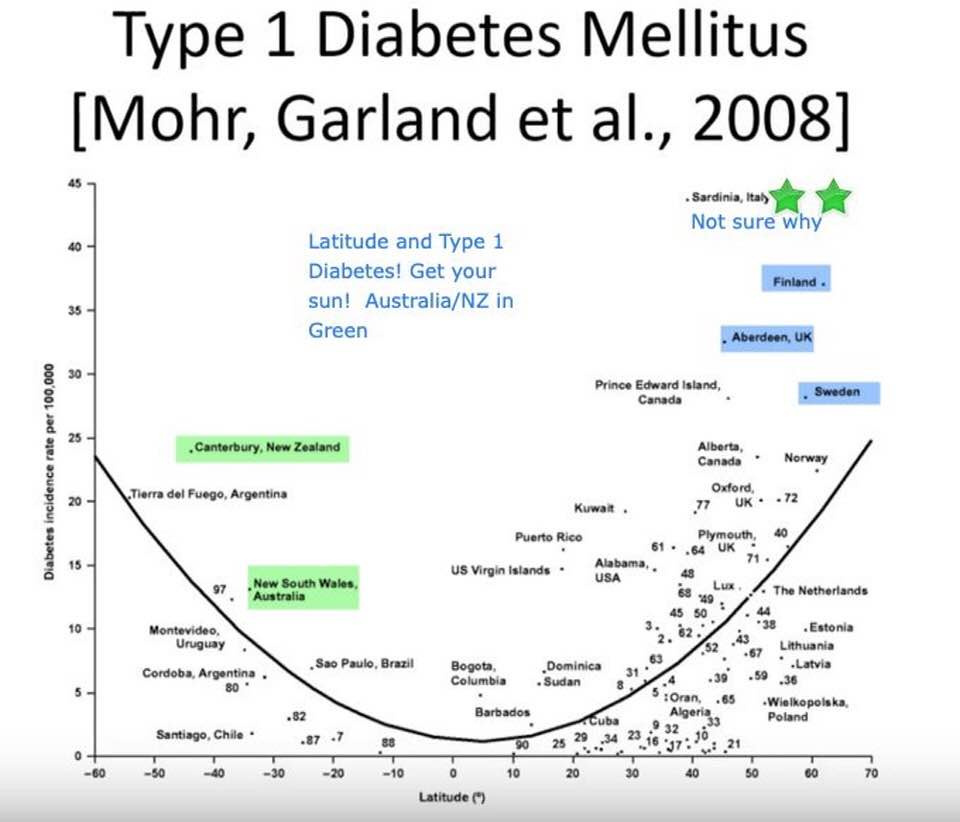
You don’t need people’s expert opinions on a fact of nature, says Mother Nature. Understanding how light from the sun is tied energy and information transfers to support this idea. The modern paradigm has carefully crafted a meme that the sun is toxic for us and this is ludicrous when you consider we have massive data that the sun reduces all cause mortality.
Hormone panels are a reflection of the cells reaction to their light environment. That is a choice you make before sex.
Adiposity and leptin resistance makes obesity a stem cell strategy rather than a disease pathology…….all driven by altered ubiquitin tied to the melanopsin and retinol mechanism.
Pregnancy is affected by electrification. If you are infertile you better join my tribe soon before you make some more incorrect choices. Infertility means you’re leptin resistant = melanopsin dysfunction due to electromagnetic interference.
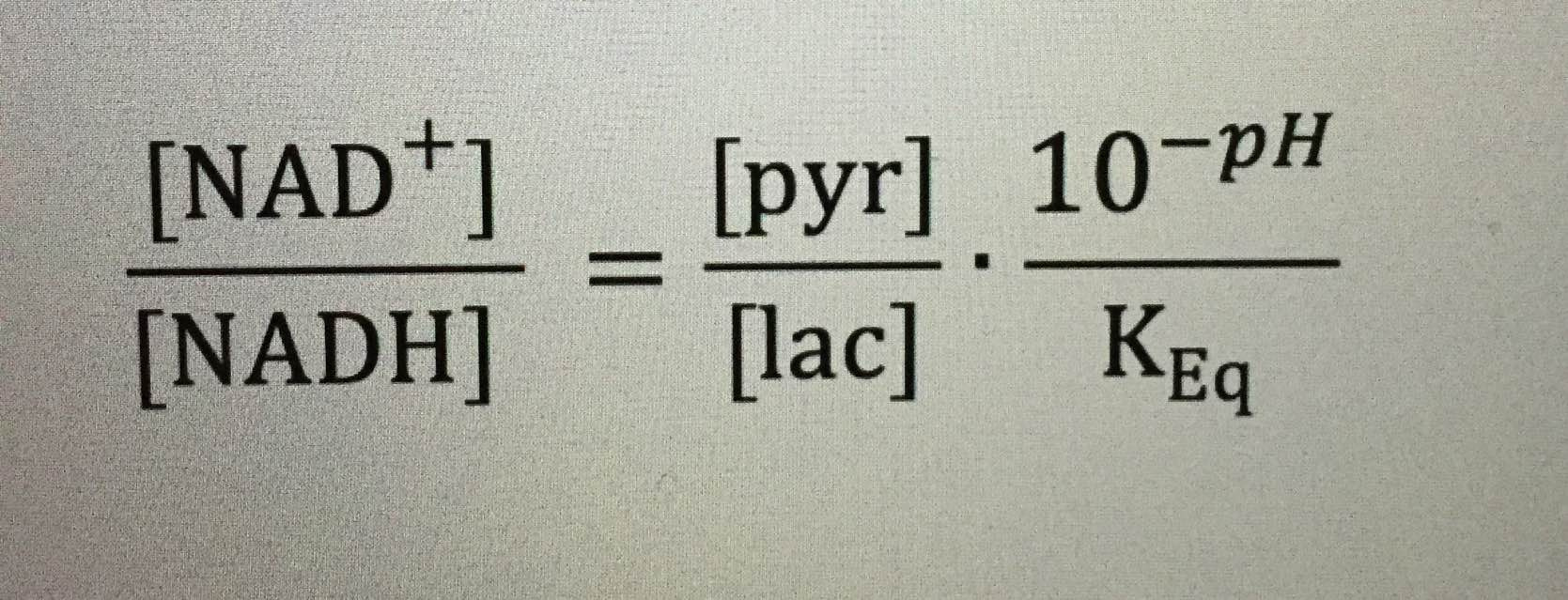
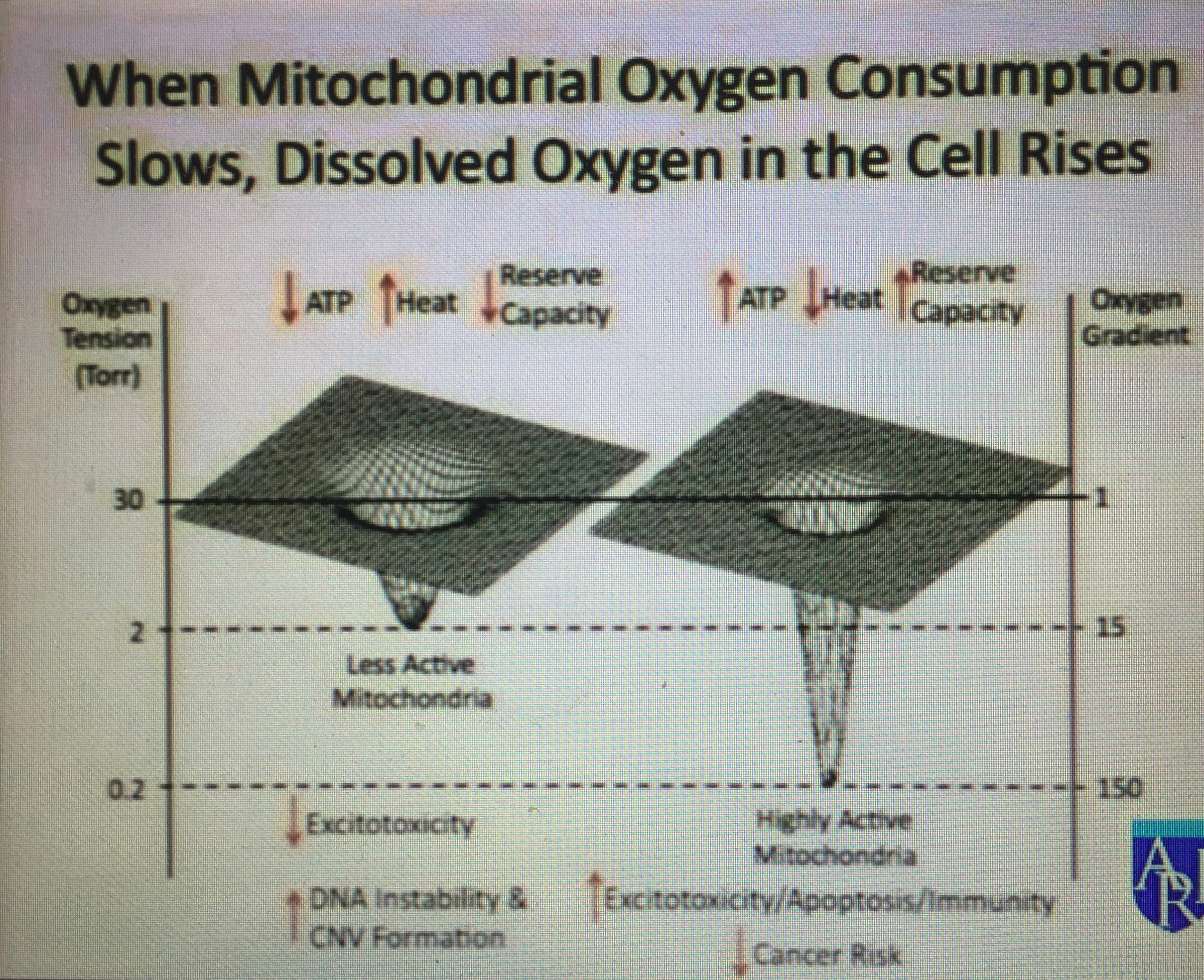
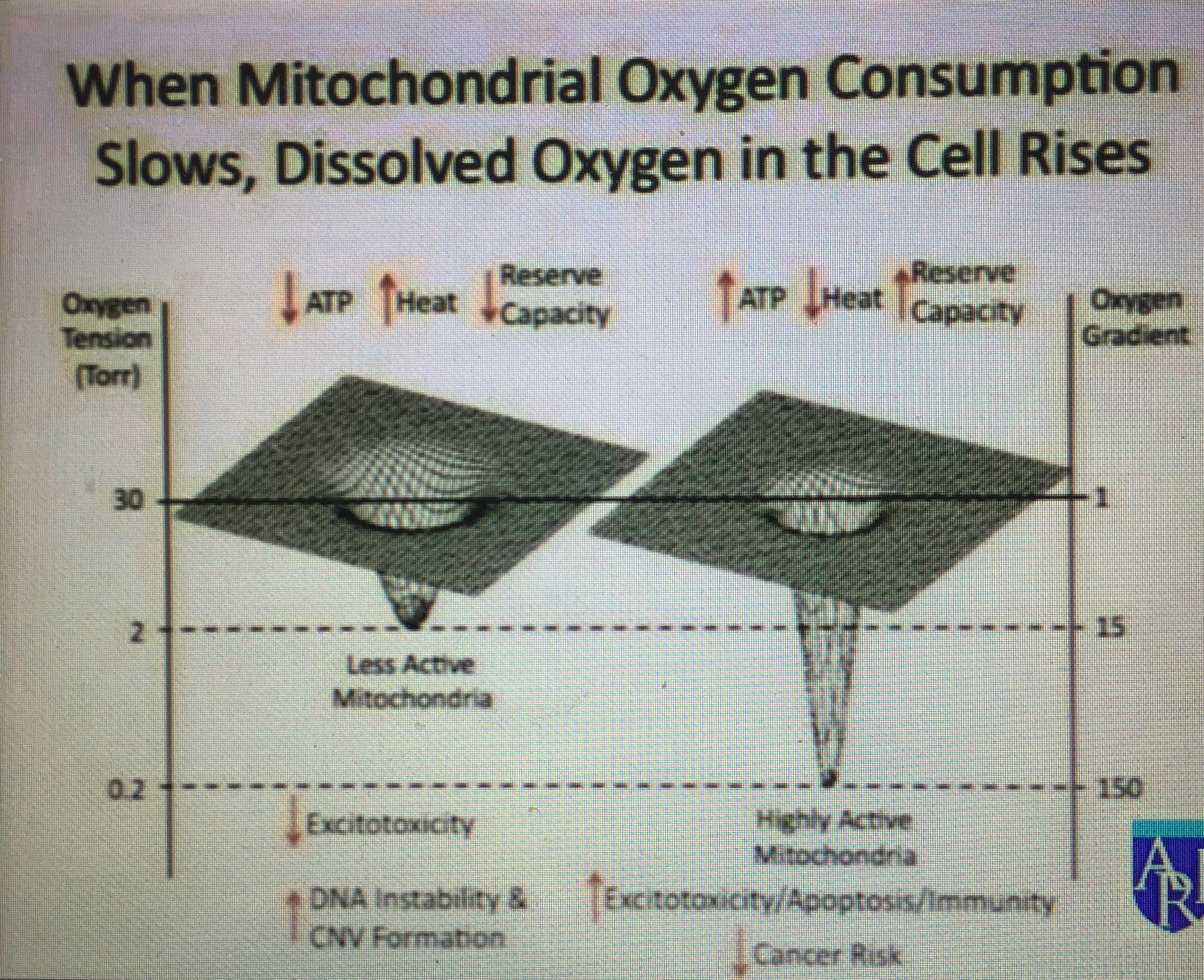
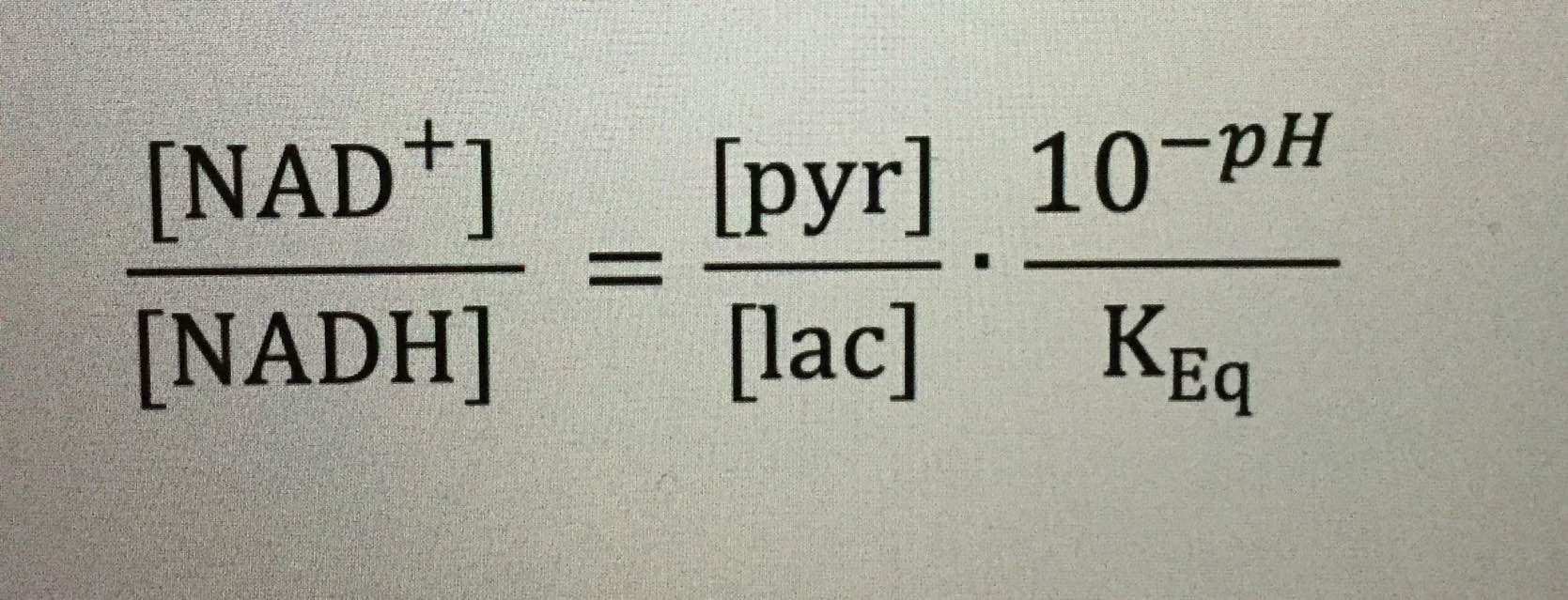
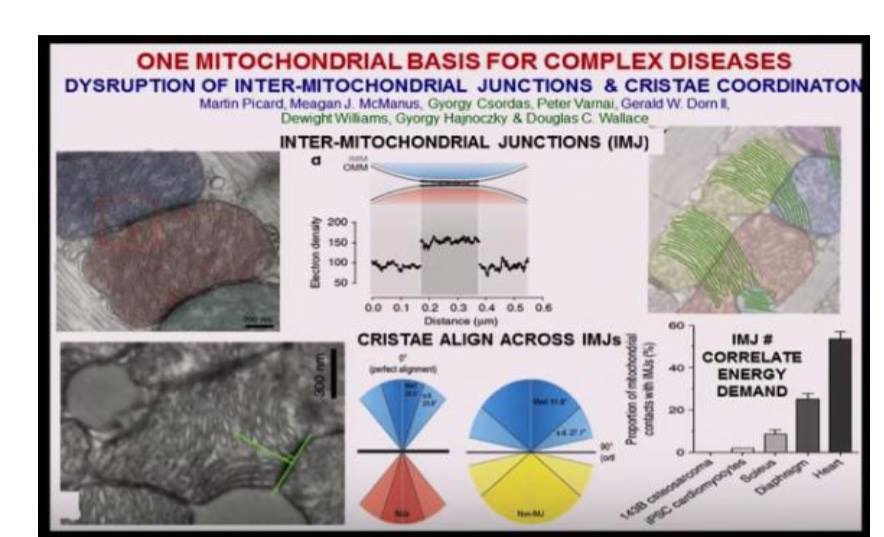
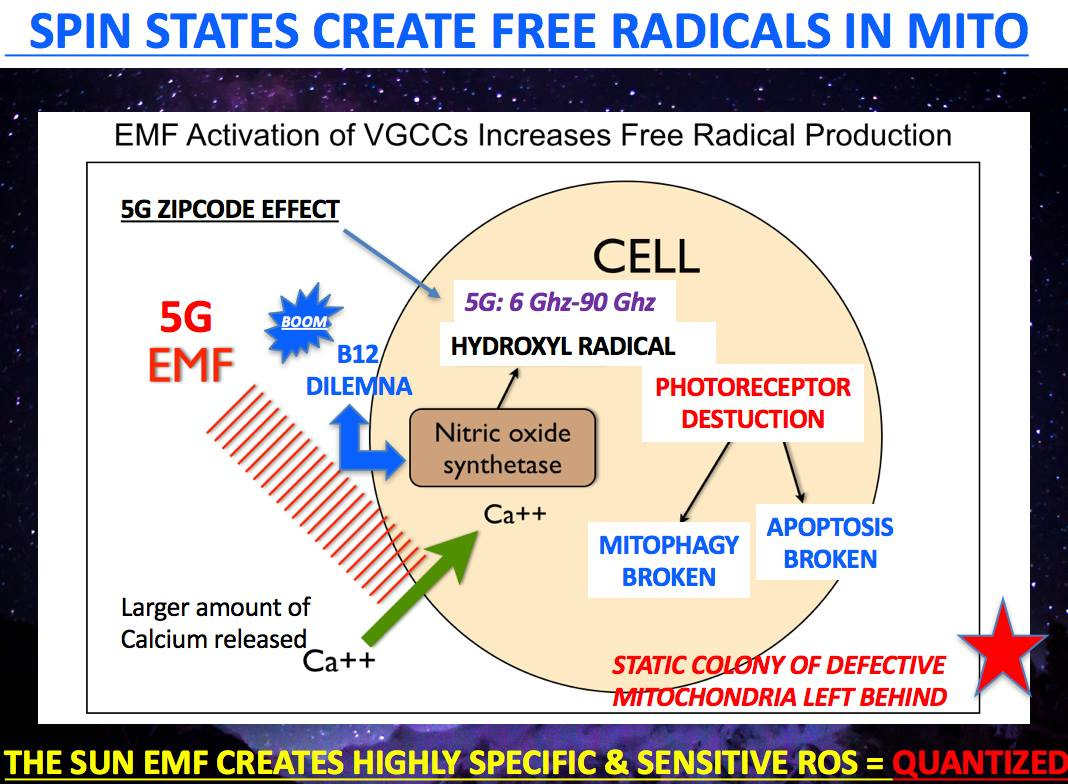
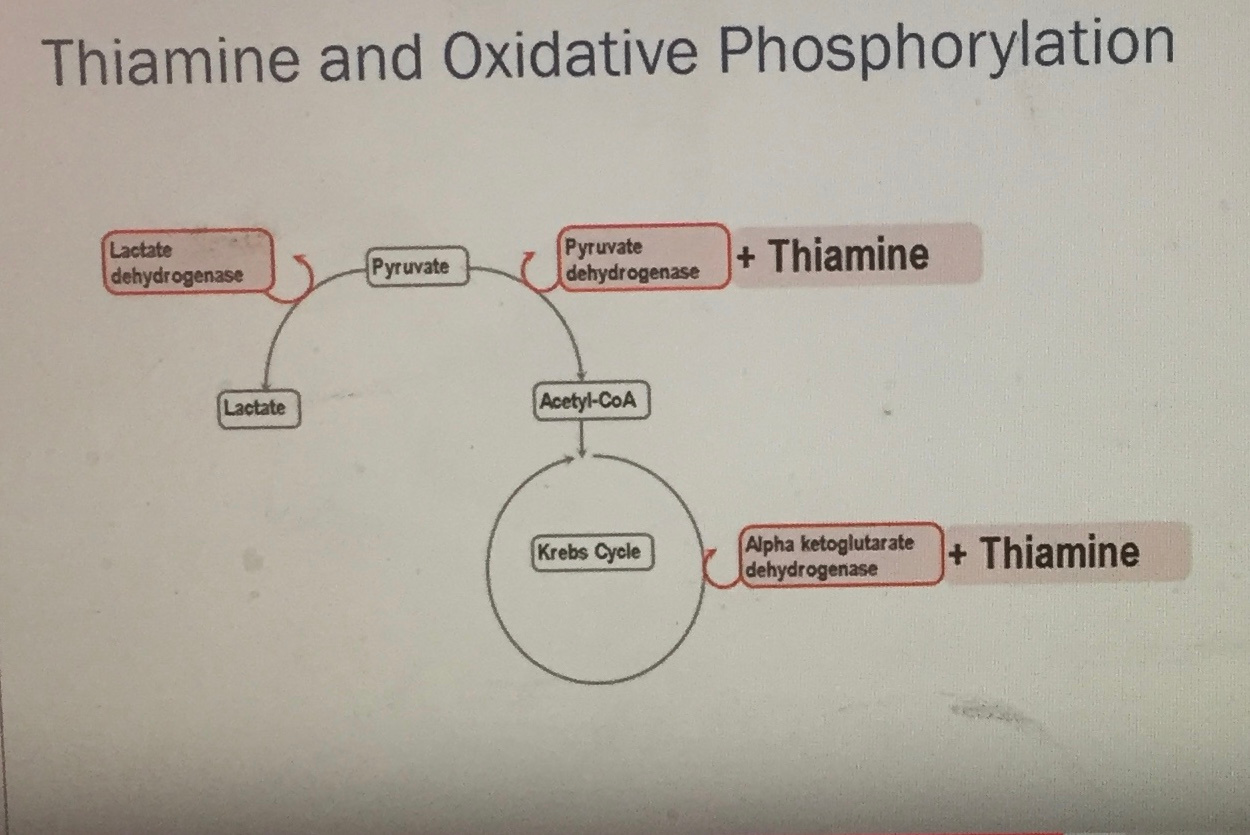
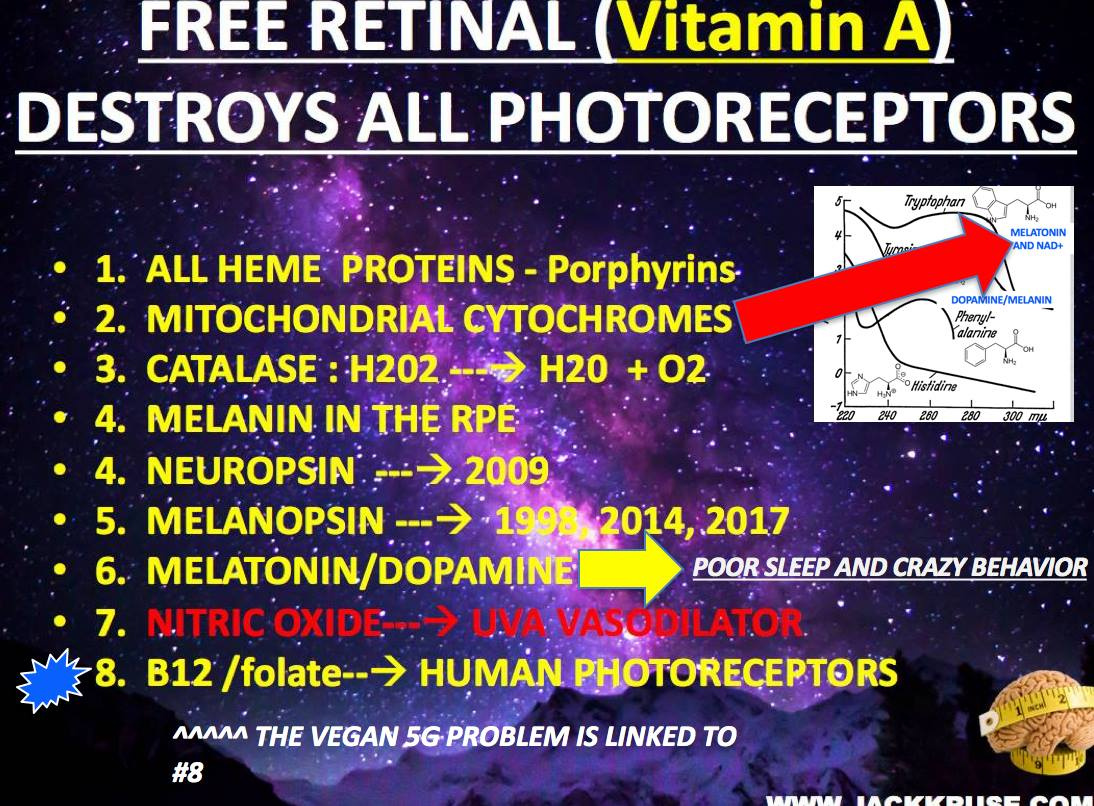
Pseudohypoxia = low O2 = Low NAD+/NADH ratio = NAD+ = altered Pyruvate/lactate levels in the mitochondria = altered matrix functioning = altered thiamine dynamics = alterations in blood sugar and AMPk pathways = altered sex steroid hormone panels = evidence of melanopisn damage = higher serum retinol = photoreceptor damage = tryptophan break down begins = the neural toxicity of the selected breakdown pathway destroy tissue and stimulates HIF-1 alpha = alters fission and fusion rate in the mitochondria = size and shape changes in the mitochondria = oxphos slows = NAD+/oxygen levels drops further in people with blue light exposure = elevated ubiquitin rates = more need for methionine and thiamine = low levels of electrons in tissues = less electrons = less solar activiation of electrons = electron density in tissues is a function of the DHA concentrations and solar exposure = less UV/IRA light = low EZ size in cell water = dehydration = higher positive charges (protons) in proteins making them less hydrophilic = low intracellular pH = low redox potential = cell and mitochondrial swelling (cyto c release) = lowered magnetic and electric fields in mitochondria = low ATP levels = a lot of carbs and protein electrons on ECT = further destruction of thiamine stores = more hypoxia = altered local and regional melatonin, serotonin and dopamine levels in the retina and frontal lobes = NT release tied to calcium efflux = calcium controls voltage gated channels, NMDA, and glutamate excitotoxicity= low DC electric current = low tissue DHA = infertility = altered perceptions of reality and depression/anxiety and just about any other disease you want to understand.
There are 3 layers to how life organizes that parallel the 3 legged stool, light, magnetism, and water chemistry. Why have I talked about pseudohypoxia for so long in this series? This is what results when we have altered thiamine levels due to chronic blue light and nnEMF exposure in our environments.
Why have I told you to go back and read David Sinclair’s Dec 2013 paper on SIRT 1, HIF 1, and NAD+? They all link to every disease on this planet. Why? The liberation of oxygen from photosynthetic plants and bacteria also allowed more complex life forms to evolve using more complex energy transfers. These waste products of two kingdoms directly allowed DHA to form in the oceans 600 million years ago. The more complex things become morphologically in an organism as evolution has evolved, the more brain one needs to control all the circadian systems tied to the environmental signals. The more oxygen in seawater, meant the more electrons would be able to collect from our environment from many sources like food, the sun, water, and our magnetic field. It also meant we could create more electrons from the endogenous electric and magnetic fields created in each mitochondrial in our cells. This slowly allowed DHA to build up in sea plants like algae and phytoplankton. Fish began to eat these plants and use DHA to build their own neural systems. The more life that evolved within the sea, meant the world’s oceans would be more green, and not blue. Green seawater = increased DHA, Iron, and O2 content. Blue seawater = little DHA, no iron, and low O2 content. Low O2 content means less magnetic energies can be utilized. This is why hypoxia is toxic to eukaryotic life at a fundamental level.
CITES:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4076149/