Pictured above is the “former” lead singer of LinkinPark. He killed himself a few years ago. His best friend Chris Cornell formerly the lead singer of Soundgarden did the same a few months before him. Was this a coincidence or was there a reason for it that modern science misses? Are these two deaths related in some way? Might it be their choice around light? Might it be their former jobs? Might it be tied to the environment their jobs required of them?
This filmed event was done at the guest house I stayed at the night before my Vermont talk. I was interviewed live in the video for 1.5 hours and I was asked questions about how blue light affected shift workers. 40 or so of my members were in attendance and one of them put this discussion on tape for you all to hear. My videographer told me this was one of the best interviews I have ever done. I’ll let you be the judge of this.
Music deaths are now so commonplace that none of them surprise us. Why is this link present in musicians? Most musicians perform at night under blue light. They use electricity to electrify acoustic instruments, sitting within that power grid and under blue light and wearing sunglasses day and night blocking their eyes from the sun over decades.
On April 14, 1994, the Seattle Post-Intelligencer reported that Cobain was “high on heroin when he pulled the trigger”. The paper reported that the toxicological tests determined that the level of morphine in Cobain’s bloodstream was 1.52 milligrams per liter and that there was also evidence of valium in his blood at 27 years old. Valium is a drug that interacts with GABA and the perihabenular nucleus in the thalamus. Is this small fact important?
Health is the slowest form of death we create in life and few realize it. Why did Soundgarden’s lead singing need the drugs he did? It was due to a lack of the protein POMC in his brain because the solar signals his brain needed never were received. When POMC is lowered, so are dopamine and melatonin. Melanopsin signaling is destroyed in both the eye and skin in musician shift workers. This alters their attitude and mood chronically too. When dopamine is low in the eye and brain so are melatonin levels in those areas too. This leads to a circadian de-coupling on a massive scale. When you add in other drugs that alter time perception like Ativan/Valium you cause a frequency collapse.

Suicide by manufactured light in this group of people becomes explainable when you see the quantum fabric of nature unfold for a brain slowly being robbed of its mitochondrial redox potential. This is why physicians are now seeing a rising suicide rate in themselves too. I loved Cornell’s music but we have to get the word out to them that acoustic and not electric music can save them. His best friend, pictured below, was famous for wearing sunglasses indoors during the day. Bennington of LinkinPark killed himself a few months after Chris Cornell. He hung himself after his drinking relapsed. Underneath his iPhone, found beside him was his bit-off fingernails. This is a classic sign of anxiety disorder. Anxiety disorders are also linked to altered signaling in the perihabenular nucleus. That is the second time I mentioned this part of the brain.

Ask yourself why this KEEPS happening in this industry? This is not a new trend. Elvis Pressley, Jimi Hendrix, Janis Joplin, and Jim Morrison all killed themselves early in their careers. Musicians have felt the need to play their concerts indoors under man-made light shows light and they love tattoo’s on their skin. They rarely play gigs outside in the sun. Does putting a tarp over your eye and skin affect the melanopsin system badly? Is this another factor in why they die by their own hand? My members know I have a very popular frontman in a well-known band as one of my key pupils. He asked me for help over 12 years ago and he reconfigured his life to avoid this tragic outcome for himself. He is now dominating his field after rebuilding his music life by controlling his light environment.
Uncle Jack tell me a bit about this PERi-HABENULAR NUCLEUS link and the human eyes
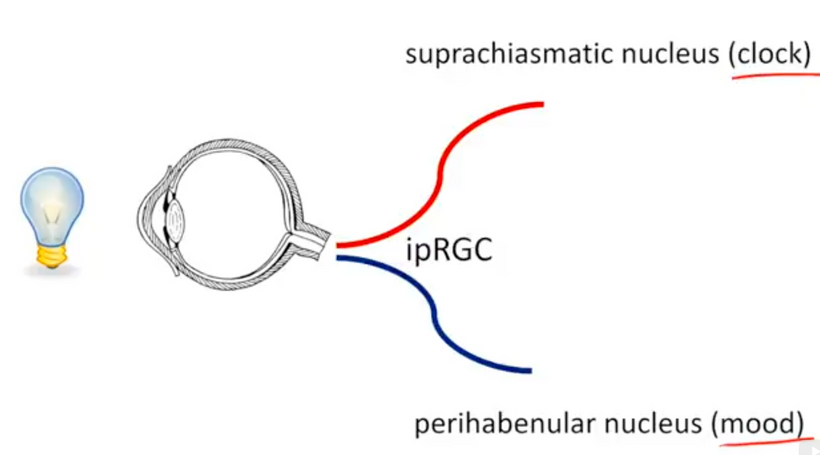
^^^^This is the basic wiring diagram through the central retinal pathways that lead to suicide by blue light.
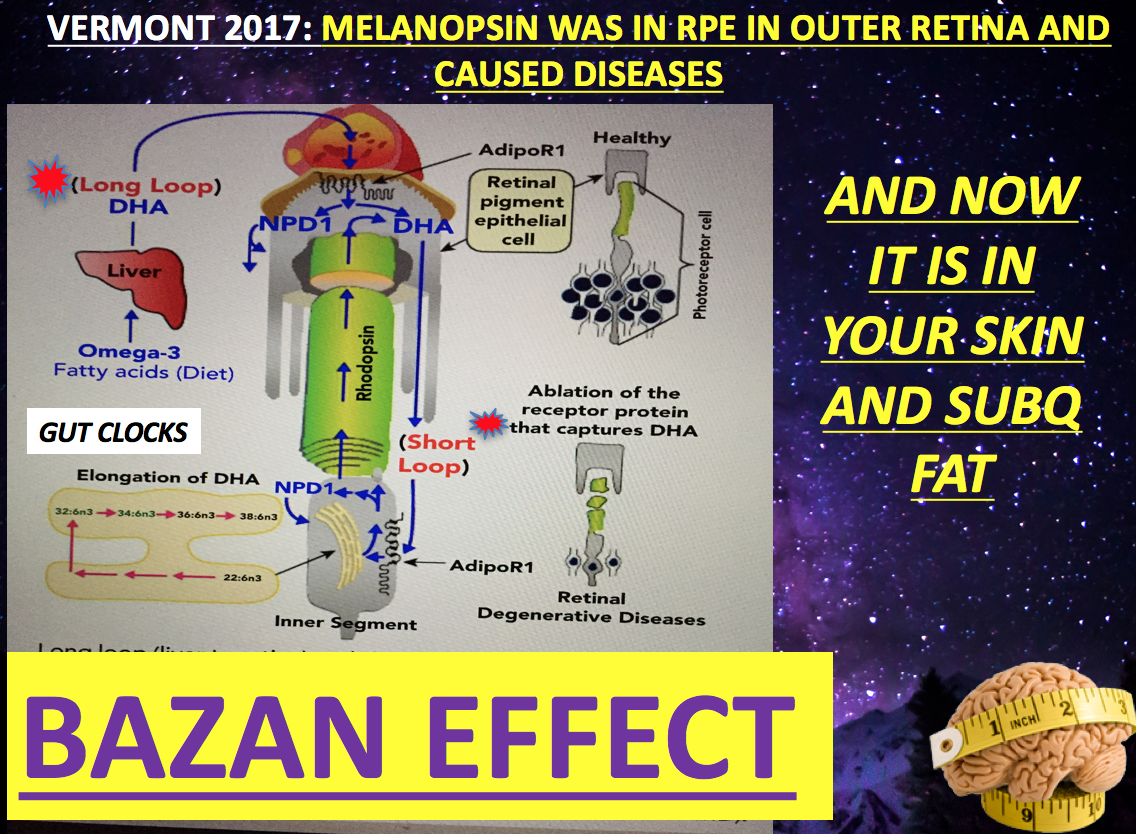
Modern Music can kill us because of how we use it and the environments it is created. Swedish DJ Avicii recently killed himself. All his gigs were done at night. He also happened to come from a high latitude steepening his mitochondrial risks. The DJ, born Tim Bergling, killed himself with a shard of broken glass from a liquor bottle, according to sources privy to details about his death who spoke with TMZ. They said there had been massive bleeding associated with the self-inflicted wound. Drinking and cutting oneself is classic behavior of a low dopamine state. His case is very interesting to me because it was linked to broken peripheral gut clocks and his melanopsin/retinol link. Avicii had a history of pancreatitis partly brought on by heavy drinking and had his appendix and gallbladder removed in 2012 before he released his debut LP. These symptoms all link back to the light he lived under as the picture from my June 2, 2018, Vermont talk on melanopsin shows below. He was 28 when he killed himself.
Modern music and modern light kill when we make it artificially and modulate its frequencies. This induces topologic changes in the charge on our skin that uncouple retinol from melanopsin that lead to a lowering of both melatonin and dopamine. This is how the path to suicide begins. That path is littered with chronic mitochondrial dysfunction and lowered mitochondrial melatonin production that leads to excessive tattooing, drug use, poor sleep, drinking, and behavioral change.

We need to go back to the basics with music. It is based upon a fractal organization to timing too. That is linked to altered dopamine levels in the eye and the frontal lobes linked to the light we abuse. That timing is linked to the human brain’s alpha waves on the EEG. When melanopsin is off so is the alpha wave on EEGs. When the alpha wave goes then we can find problems in others waves that signify a sleep disorder. This sleep disorder always precedes sickness, suicide, and death.
Can we see the evidence of light toxicity in the skin before it afflicts the brain? Yes, we can. People often forget that the skin and brain comes from the same tissue layers in the human embryo. Because of this linkage your skin and your eyes tells your decentralized physician to look deeper into your health to see how bad you are afflicted with light toxicty.

This is a before and after picture of someone who was light toxic and became light competent under the direction of a a decentralized mitochondriac physician.
Michael Jackson is a perfect example of this dynamic effect below. Sunglasses at night under a massive light show. He also had melanopsin induces autoimmune skin condition called vitiligo. Vitiligo is improved by full-spectrum UV light. This is light he rarely saw as an adult. Jackson died after convincing a physician to use IV Diprivan on him to allow him to sleep. He suffered from chronic insomnia for decades = lack of melatonin creation inside his colony of mitochondria = lack sunlight = extreme blue light toxicity.

The trend continued with Whitney Houston in her life with drugs and poor sleep. How many young people do we need to see die in the same way before we make the links of why this happening? This is why acoustic music can soothe us and why electrified music can cause massive spiking of evoked potentials that lead to addiction, depression, and suicide. Technology in music brings man inside out of the sun and we’ve created music shows to occur mostly at night when our retinal photoreceptors that provide the light stimulus to make POMC via the eye and in our brain is destroyed. Sunlight creates happiness and keeps us far from moods that lead to a self-induced death with pills, opiates, or a rope. The human brain has many waveforms and frequencies cycling at different rates simultaneously. Moreover, many, if not all, contribute to one’s internal experience of time. This sense is controlled by dopamine levels and how its frequency in circuits in the brain. Consider the death of Heath Ledger after his role as the Joker in Batman. Most of the film was done at night and by all reports, his drug and alcohol use expanded while his reality about the role became very warped in delusion. That led to him taking his own life at 28 years old. It does not take very long to see the effect of a broken melanopsin system in the central retinal pathways in humans if you know the signs and symptoms.

Suicide by light is linked to a loss of the internal experience of time in the brain because dopamine is missing. nnEMF can cause massive spikes and losses of evoked potentials in the brain because it decouples calcium channels. Most people do not even know the blue light chromophore in our eyes and skin called the Melanopsin/retinol mechanism that runs on calcium ion flows. Ativan and opiate drugs like this exacerbate the condition. Ativan affects GABA levels in the brain. Ativan is the drug that was found in Soundgarden Chris Cornell and Cobain’s blood plasma after they killed themselves.

When dopamine/melatonin are lacking we can perceive and sense the fractal side of nature. Many mental illnesses are associated with a low dopamine state and those patients report a frozen existence of reality. In those frozen states, humans become able to do things humans normally would not do. Many depressed patients describe their life seems like ‘still photos’ of a flickering vision, like a movie film that is running too slow on the screen. The ability of the brain to keep all these different frequencies in appropriate relationship and order to one another, smoothing the flow of connecting thoughts and actions, is what dopamine helps facilitate. Photons of light come to Earth and to humans in a timeless state. Our brain gives us the sense of time by coupling light frequencies to build time. Dopamine and melatonin are two gears of that mechanism. These chemicals are the “matter” that nature uses as its levers.
It takes matter in cells to create time using UV light photons. By themselves, photons would perceive the world, as frozen. Light photons have an interior temporal indivisibility that prevents the perception of external divisibility. We now know UV light is critical in the creation of dopamine in our eyes with aromatic amino acids which act as photon traps for the timeless light of the sun. Chris Cornell’s lifestyle around his job chronically buried the sun and created a need for drugs because of the missing frequencies…………and therein lies the true story of his demise. This video interview, below, is all about this topic in the music business I did a few years ago before one of my Vermont live talks. Watch it and share it with those you love. Few of us make these connections to the light we live under.
Here is the powerful video laying out the case of why this process happens to shift workers at night.
https://www.patreon.com/posts/blue-light-skin-19980836
THE SCIENCE IN THIS BLOG BECAME CLEAR IN 2016-2018 that the eye was the key.
Can you share with us a disease that shows how light chaos destroys order in cells?
Sure, the one that is becoming all too common is steroid induced psychosis.
When I was a young physicians this disease was really rare. Today it is becoming very common because of the use of tech screens, indoor living, and a lack of solar exposure.
Centralize medicine does not understand this disease well at all. The reason for that is they do not understand how the retina was built, and how light creates time from light.
THE QUANTUM BIOLOGY ANGLE
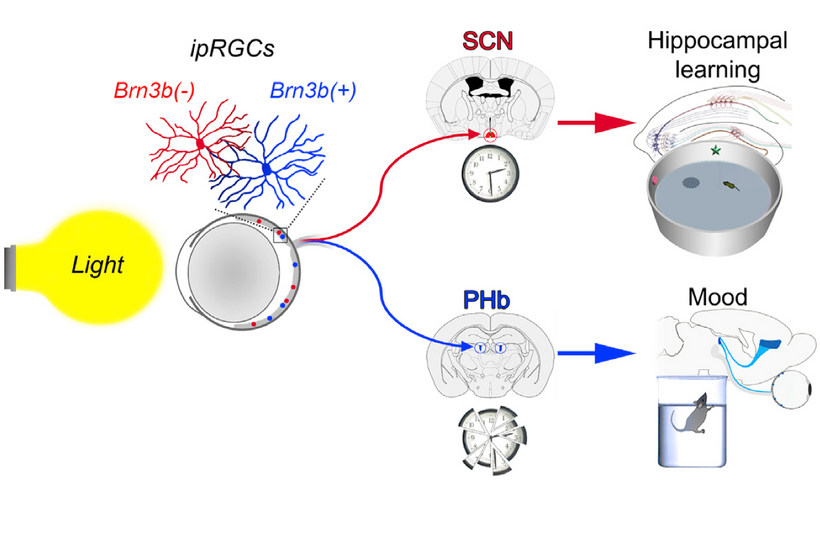
The effects of light on learning and mood via intrinsically photosensitive retinal ganglion cells involve a pacemaker- independent role for the suprachiasmatic nucleus as well as distinct circuitry in a region of the thalamus called the perihabenular nucleus.
It appears there are two distinct central retinal brain pathways that mediate the effects of light on learning and mood in mammals. (below)
In mammals, light detection occurs exclusively in the retina. In addition to classical rod and cone photoreceptors, a subpopulation of retinal ganglion cells (RGCs) that express the photopigment melanopsin (Opn4), making them intrinsically photosensitive (ip)RGCs, constitute the third type of photoreceptors besides rods and cones.
At present, 5 subtypes (M1–M5) of ipRGCs have been described in the literature. Their central projections differ amply, reflecting in this variety the multiform nature of the non-image-forming visual functions they participate in such as circadian photoentrainment and sleep regulation. A major ipRGC target is the hypothalamic suprachiasmatic nucleus (SCN), which houses a central pacemaker that orchestrates peripheral clocks to drive circadian rhythmic coherence. (eye clock)
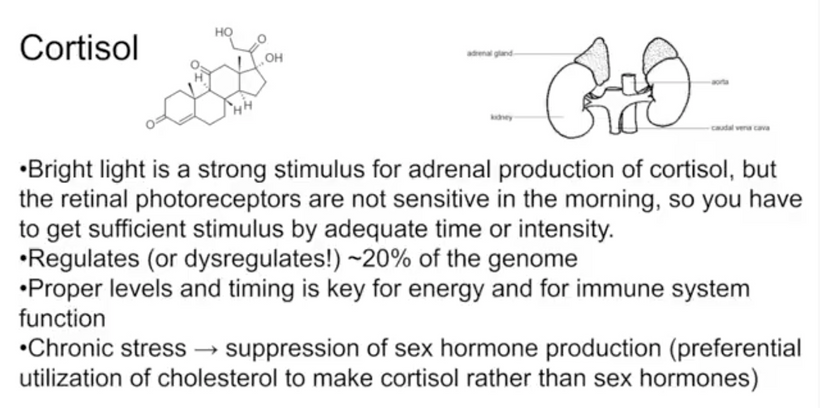
The pathophysiology of this disorder is poorly understood but it follows many other mitochondrial diseases that result in altered cortisol levels from blue light over exposure and solar light under exposure. This is why it is more common in modern times. Other diseases like Cushing’s or Addison’s are well known to be associated with abnormalities of the hypothalamo-pituitary- adrenal axis and have the potential to result in mood disorders by disturbing the cortisol pathway as the synthetic steroids activate.
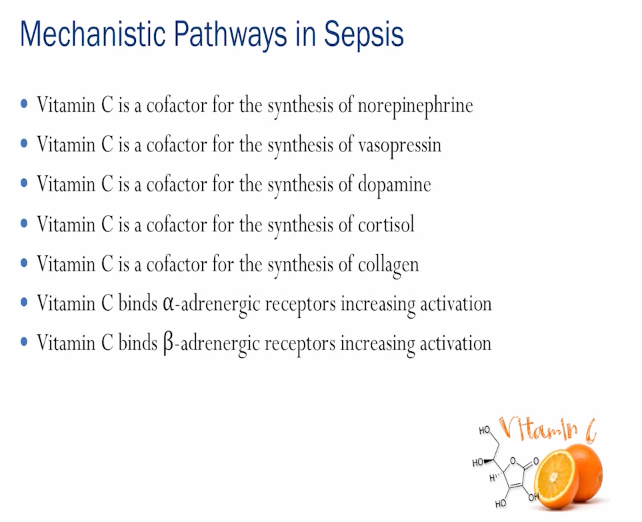
Vitamin C is used up more rapidly when sunlight is missing or exogenous steroids are given to some one. In fact, any stressor to the system causes rapid decline in the chemicals below. That decline in part is why pregnenolone steal syndrome occurs in humans under duress.
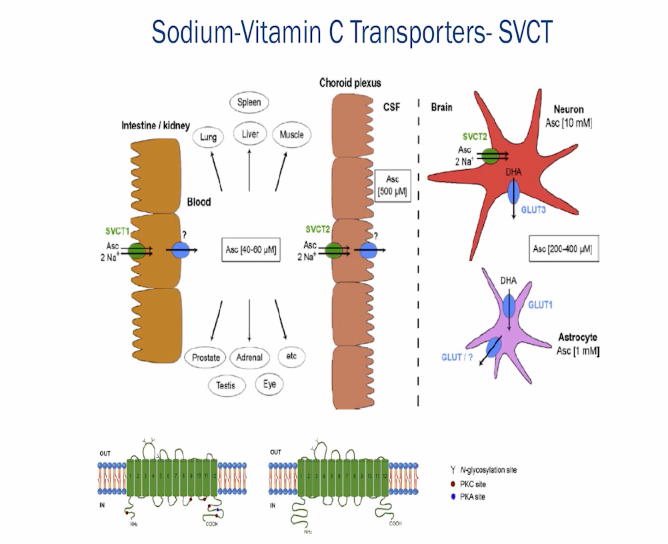
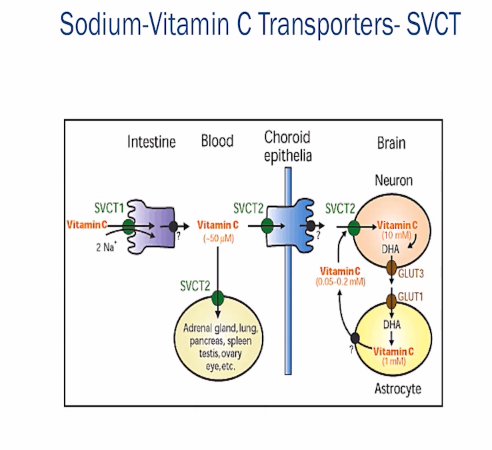
Vitamin C is a metabolic switch in the human brain: glucose and lactate metabolism are modulated by ascorbic acid. Ascorbic acid is highly concentrated in the human CNS. All stressors increase glutamate in the human brain. Why is this? For this switch to occur, an ascorbic acid flow is necessary between astrocytes/glia and neurons, which is driven by neural activity and is part of vitamin C recycling.
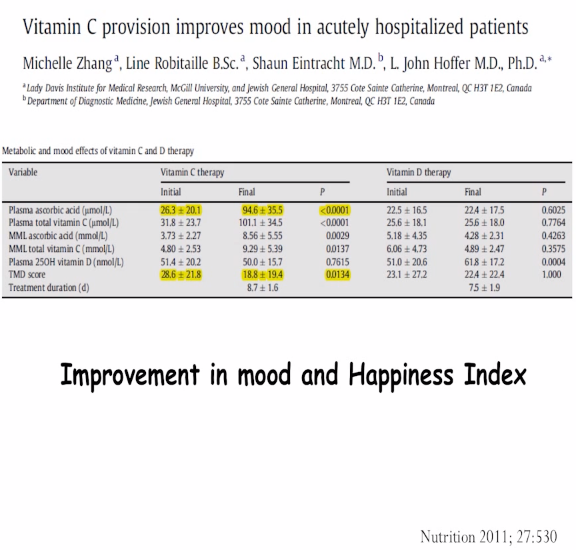
Glutamate release from from neurons that are light/cortisol stressed, stimulate ascorbic acid release from astrocytes. This can deplete the brain of vitamin D. When Vitamin C drops you brain needs to use glucose metabolism to operate and it is not efficient to do so. Ascorbic acid entry into neurons and within the cell inhibits glucose consumption favoring the use of ketones and they do this by stimulating lactate transport. The take home: everyone who is light stressed has very low CNS Vitamin C levels and Vitamin C levels in the brain can only be replated by SVCT2 receptors in the blood stream and not from the gut which relies on SVCT1 and is saturable at 1000-1500 mgs per day. The SVCT2 receptor has no limit on absorption in health. It is down regulated when inflammatory cytokines are present. (stressors all cause increased cytokines) See the pics below to make this case for you.
THE KEY POINT IN THIS BLOG BELOW
So what do decentralized MDs know that centralized MDs never learned? Mood regulation by light requires an SCN-independent pathway linking the ipRGCs melanopsin cells in the retina to a previously unrecognized thalamic region, termed perihabenular nucleus (PHb).
One of the things I have noticed over the last 15 years in this diseases is that all the people who became psychotic with exogenous steroid use all had weak pupillary responses to blue light. It was secondary to the slow destruction of dopamine and melatonin in the skeletal muscle of the pupil that controls its function. As both of the chemicals were lowered by blue light the skeletal muscle fiber type of the pupil changed and made the pupillary muscles atrophy and become sluggish in their response to blue light. Why is the pre-condition important in steroid induced psychosis?
The answer is buried in the picture above. The central retinal pathways that project to the SCN have to be disrupted when the pupil is sluggish in its response to the blue light stimulus. This also means that the neuronal projections to perihabenular nucleus in the thalamus are also disrupted and lead to mood disorders. When these two clinical signs are present, the decentralized clinician knows immediately that light toxicity is an envionmental player harming the patient. It is a sure sign blue light or nnEMF has disturbed neuronal signaling and metabolism in the cortisol pathways of the brain. Below is a coronal cut T1 MRI of the brain showing this region.
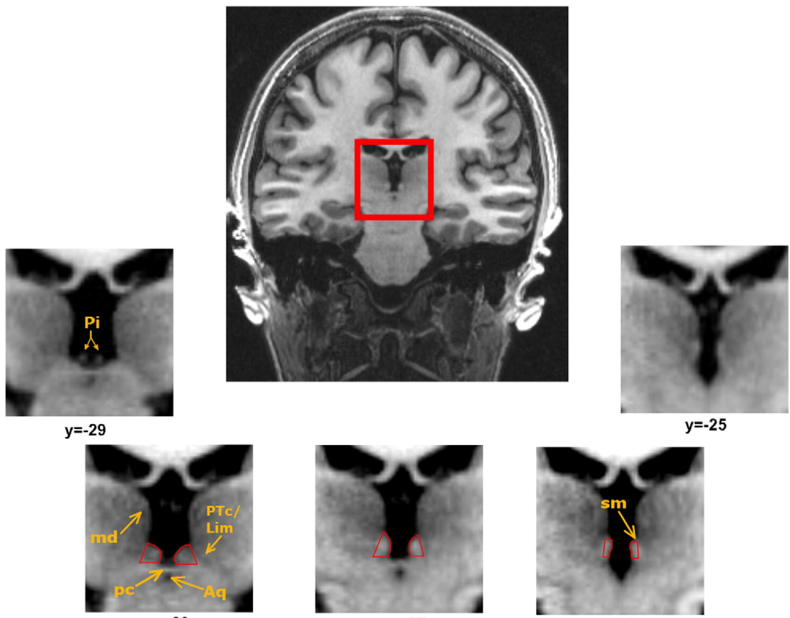
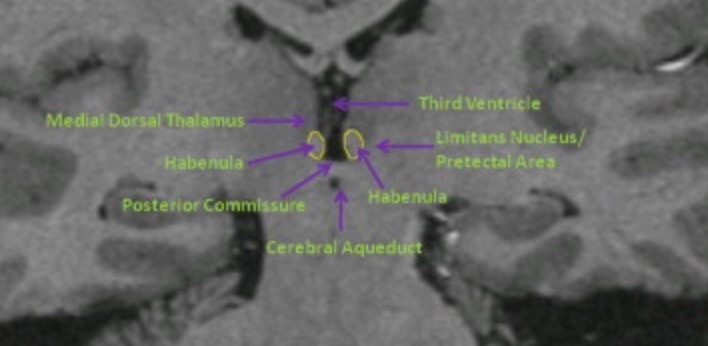
The habenula is a complex nucleus in the thalamus of humans composed of lateral and medial subnuclei, which connect between the limbic forebrain and midbrain in the brainstem as shown below. Over the past 5 years, the lateral habenula has received considerable attention because of its potential roles in cognition and in the pathogenesis of various psychiatric disorders.
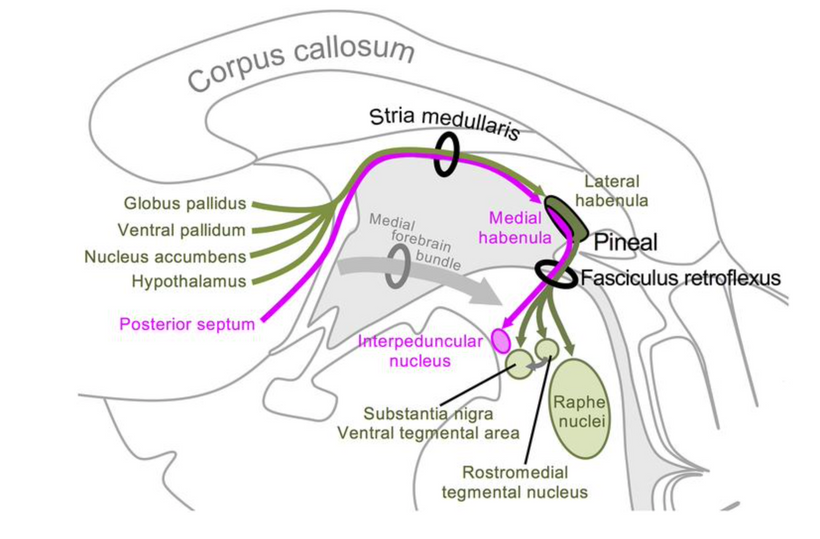
The habenula is an evolutionarily conserved structure in the brain and regulates the central monoaminergic metabolism in humans. Disturbances in monoamine metabolism include a depletion of norepinephrine and suppression of central dopamine in the brain. This region likely a light relay center for the brain. It is very close to the pineal gland and the collicular plate which links it to all things visual. This is why eye changes tells us about the brain’s toxic light effects. Despite a surge of interest on the habenula in neuroscience since 2016, function of the human habenula remains murky.
For example, the medial habenula is the source of one of the major cholinergic pathways in the brain, relatively few studies have been conducted to understand its roles. When acetylcholine is destroyed in the brain cognition drops and low ACh is associated with Alzheimer’s disease. I believe this is how AD begins and develops.
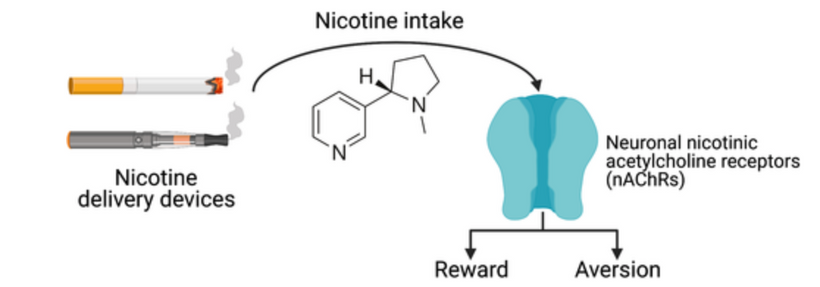
Nicotine addiction operates here as well. This is why I believe people who wear blue blocking glasses find the use of nicotine difficult over time. People who are blue light toxic almost seem immune to it. This is another clue I use in Kruse Longevity Center Farm patients during their work ups to know how badly they are light toxic.
I believe this nucleus hold the clues to many diseases including depression, bipolar disorder, and Parkinson’s disease. I also believe this pathway is acutely disrupted in people who use exogenous steroids when their brains are low in Vitamin C due to light stress. Giving these patients synthetic steroids, while they are blue light toxic, hyper activates glucocorticoid receptors preferentially in the SCN, PHb, and the hypothalamus simultaneously, which suppresses the secretion of cortisol by the adrenal glands.
This is why most modern humans have flat lined cortisol cycles when one checks the cortisol levels for them. Decentralized MDs know to look for it, and centralized MDs think this is quackery because they are ignorant of the neural wiring diagram above from retina to brain.
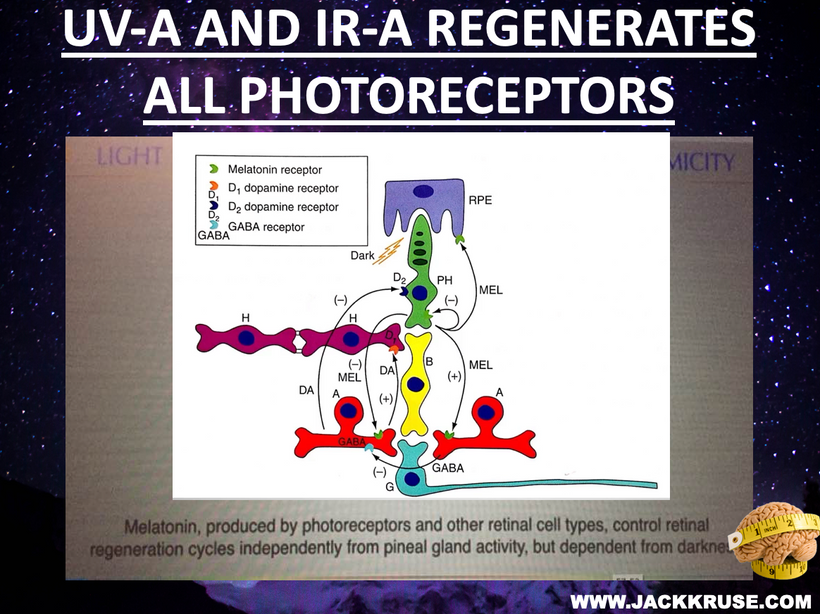
The slide above tells you how the pathophysiology develops. The chronic blue light exposure ruins the regeneration of the ipRRGs in the retina. They rely on optimized dopamine and melatonin levels to keep our timing mechanisms via the SCN intact. When the photoreceptors cannot regeneration mood disorders can also manifest because of the disruption of the tracts from the IpRCGs to the perihabenular nucleus.
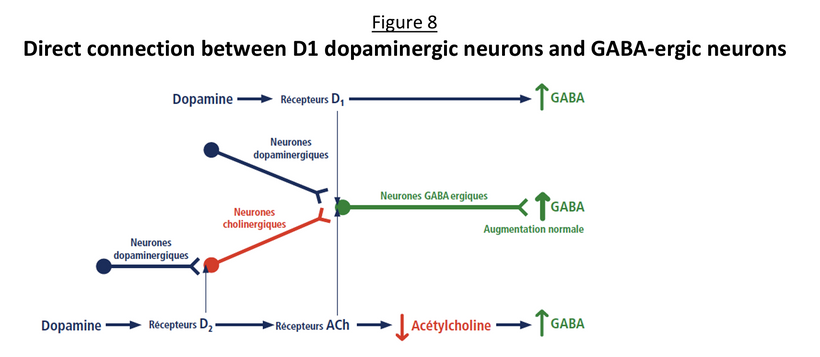
The slide above shows when dopamine control is lost in the central retinal pathways, GABA also will be lowered in the brain. Remember what I said about all the musicians above who killed themselves? They were also abusing GABA like drugs. Most of them smoked as well. Now you might understand why they were doing it now. What else happens? Acetyl choline receptors will drop and as this happens, acetylcholine levels will rise in neural circuits to also lower GABA.
A deficiency in ACh receptors and lowered dopamine levels can mimic myasthenia gravis (check my MG blog on patreon out) with poor muscle tone. A deficiency in GABA activity can contribute to certain mental health conditions such as anxiety disorders, schizophrenia, and depression. It’s also involved in some physical conditions, including Huntington’s disease, dystonia, and muscle spasticity. Low dopamine levels are also associated with mood disorders like depression. These deficits all get worse and eventually are all present at the same time when the human brain begins to contemplate taking its own life.
When you are given exogenous steroids and you do not get enough sunlight, it is the perfect storm to getting steroid induced psychosis. This is a key point why a lack of sunlight or too much exogenous steroids cause the same problem = MENTAL ILLNESS
CASE DESCRIPTION OF STEROID INDUCED MENTAL ILLNESS
A 35-year-old man information technologist who works in the computer data with prior hypertension (low NO), hyperlipidemia (Low Vit D level), chronic testicular pain, lumbar spinal stenosis and radiculopathy, depression, anxiety, and post-traumatic stress disorder presented to the emergency department, after cutting into his right scrotum because he had seen someone in his shower the previous night, and “they put something in my testicle.” He had taken a kitchen knife to try to remove it. His wife called 911 for his unusual behavior. He stated that there were “bad guys trying to shoot him in the face” and that teams of doctors had “implanted a tracking device in his testicle.” During police response, the patient was noted to be aggressive toward the officers to the point where he had to be pepper-sprayed and handcuffed.
On arrival to the ER, the patient was noted to have his right testicle protruding from a 2-cm scrotal laceration and continued to have persecutory and aggressive behaviors, for which he was placed in restraints and on an order of emergency detention. While in the emergency department, the patient was observed to be oriented to his name, situation, and place but believed the year to be 2009.
His vitals were notable for tachycardia of 120 beats/min. Laboratory results were notable for leukocytosis (white blood cell count of 17.1 (high) 109/L (high)), glucose level of 252 mg/dL, and slight elevations in potassium, aspartate aminotransferase, and alanine aminotransferase. Tests for alcohol, acetaminophen, and salicylates were negative, and the urine drug test was positive for opioids, which was explained by his prescription for tramadol.
On mental status evaluation by psychiatry, the patient was noted to be calm, cooperative, and attentive. He had good eye contact but sluggish pupils to penlight exam. His speech was spontaneous, fluent, and coherent with normal rate and volume. He was alert and oriented to person, place, and situation. He had no aggressive or self-harm behavior.
His mood was reported as “frustrated” and his affect was rather calm. His thought processes were linear and goal directed. However, his thought content was delusional. He denied suicidal or homicidal thinking, intentions, or plans or thoughts of wanting to hurt self or others. He denied auditory or visual hallucinations. He did not appear to respond to internal stimuli. He appeared to have limited knowledge. His family says he he had become cognitively dulled during this event (hippocampus turned off). He displayed paranoid thought content. Insight into his problems was limited. Judgment was also limited.
Urology was consulted and his testicle was reduced back into his scrotum and the laceration repaired. He was recommended for inpatient psychiatric hospitalization at an outside hospital for his delusions. The whole psychotic episode lasted approximately 24 hours.
On further inquiry, it was noted that he had been seen the previous day at the pain medicine center for chronic genitofemoral neuralgia (testicle pain) and had received an injection of 5 mg of dexamethasone and 0.25% of bupivacaine, along with radiofrequency ablation. He had received steroid injections in the past, even just 2 months earlier, of 15 mg dexamethasone for chronic back pain.
His home medications included bupropion, fluticasone, methocarbamol, olopatadine, pregabalin, testosterone cypionate injection (pregnenolone steal), and tramadol. He was in a stable marriage with three children without any legal troubles. He was a previous smoker, having quit 5 years earlier after 7 years of <0.5 packs per day; he used alcohol socially but used no drugs.
The differential diagnosis at the time included drug use/intoxication (a urine drug test was positive for opioids but the patient was noted to be on tramadol); electrolyte imbalance (abnormalities noted but explained by gross hemolysis); infection (elevated white blood cells but otherwise no signs of infection); hypoglycemia/hyperglycemia (glucose elevated but not at a level typical of diabetic ketoacidosis or a hyperosmolar hyperglycemic state); and psychiatric causes (recent steroid injection, history of psychiatric disease).
CENTRALIZED VS DECENTRALIZED MDs are the key to diagnosis?
The chronic blue light toxicity lead to suppression of the secretion of cortisol by the adrenal glands. This preferential selection creates imbalance between glucocorticoid stimulation over mineralocorticoid receptor stimulation, leading to cognitive impairment and emotional disturbances.

Lewis and Smith reviewed 79 cases of steroid-induced psychosis and found that disturbances in reality testing were reported in 71% of the 79 cases, but only 14% had a psychotic disorder without evidence of significant mood changes or features of a delirium. They found that depression was present in 40.5%, mania in 28%, a mixed state in 7.5%, and delirium in 10% of these cases. Another study found that mania and hypomania were reported most commonly (in 35% of cases), followed by depressive symptoms in 28% and psycho- tic reactions in 24%. The vast majority of these patients develop symptoms <2 weeks from the inductive event and more typically 3 or 4 days after the initiation of corticosteroid therapy, although symptoms can occur at any time, including after cessation of therapy. The symptoms may last anywhere from a few days up to three or more weeks. In most cases, any associated delirium commonly resolves within days and psychosis within a week, though depression or manic symptoms may last up to 6 weeks after discontinuation of steroids.
There are not largely powered studies in the field of steroid-induced psychosis due to its unpredictable nature, but it is an important consideration because it is a stressful and dangerous situation for a patient to experience. Diagnosis hinges on clinician experience by exclusion, and prevention hinges greatly on keeping dosages as low as possible and not prolonging medication regimens beyond what is required.
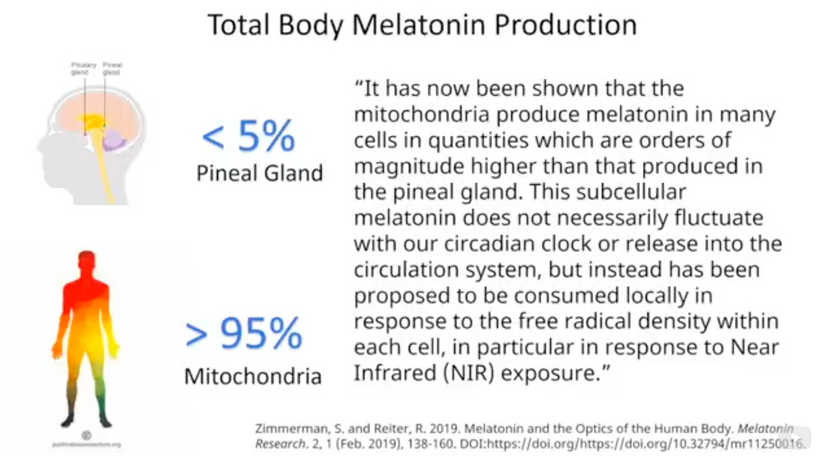
Melatonin production in your mitochondria from the red light in the sun is the key reason why most circadian/mitochondrial diseases occur.
The use of exogenous steroids acutely in people mimics the effect of blue light toxicity in humans who abuse blue light chronically. Both cause mental illness on different time scales. The reason it happens is how the retina is wired to the melanopsin photoreceptors. Now you are much wiser than your centralized MDs who still remain impotent to explain these complex phenomena to families of people who took their own life.
CITES
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Publishing; 2013.
2. Judd LL, Schettler PJ, Brown ES, et al. Adverse consequences of glucocorticoid medication: psychological, cognitive, and behavioral effects. Am J Psychiatry. 2014;171:1045–1051. doi:10.1176/appi.ajp.2014.13091264.
3. Gagliardi JP, Muzyk AJ, Holt S. When steroids cause psychosis. Rheumatologist. 2010. https://www.the-rheumatologist.org/article/ when-steroids-cause-psychosis/.
4. Lewis DA, Smith RE. Steroid-induced psychiatric syndromes: a report of 14 cases and a review of the literature. J Affect Disord. 1983;5: 319–332. doi:10.1016/0165-0327(83)90022-8.
5. Sirois F. Steroid psychosis: a review. Gen Hosp Psychiatry. 2003;25: 27–33. doi:10.1016/S0163-8343(02)00241-4.
6. Kenna HA, Poon AW, de los Angeles CP, Koran LM. Psychiatric complications of treatment with corticosteroids: review with case report. Psychiatry Clin Neurosci. 2011;65:549–560. doi:10.1111/j. 1440-1819.2011.02260.x.
7. Warrington TP, Bostwick JM. Psychiatric effects of corticosteroids. Mayo Clin Proc. 2006;81:1361–1367. doi:10.4065/81.10.1361.
8. Altimus, C.M., Guler, A.D., Villa, K.L., McNeill, D.S., Legates, T.A., and Hattar, S. (2008). Rods-cones and melanopsin detect light and dark to modulate sleep independent of image formation. Proc. Natl. Acad. Sci. USA 105, 19998– 20003.
9. Berson, D.M., Dunn, F.A., and Takao, M. (2002). Phototransduction by retinal ganglion cells that set the circadian clock. Science 295, 1070–1073.
10. Chen, S.-K., Badea, T.C., and Hattar, S. (2011). Photoentrainment and pupillary light reflex are mediated by distinct populations of ipRGCs. Nature 476, 92–95.
11. Ecker, J.L., Dumitrescu, O.N., Wong, K.Y., Alam, N.M., Chen, S.-K., LeGates, T., Renna, J.M., Prusky, G.T., Berson, D.M., and Hattar, S. (2010). Melanopsin expressing retinal ganglion-cell photoreceptors: cellular diversity and role in pattern vision. Neuron 67, 49–60.
12. Fernandez, F., Lu, D., Ha, P., Costacurta, P., Chavez, R., Heller, H.C., and Ruby, N.F. (2014). Dysrhythmia in the suprachiasmatic nucleus inhibits memory processing. Science 346, 854–857.
13. Fernandez, D.C., Chang, Y.-T., Hattar, S., and Chen, S.-K. (2016). Architecture of retinal projections to the central circadian pacemaker. Proc. Natl. Acad. Sci. USA 113, 6047–6052.
14. Guler, A.D., Ecker, J.L., Lall, G.S., Haq, S., Altimus, C.M., Liao, H.-W., Barnard, A.R., Cahill, H., Badea, T.C., Zhao, H., et al. (2008). Melanopsin cells are the principal conduits for rod-cone input to non-image-forming vision. Nature 453, 102–105.
15. Hammar, A., and Ardal, G. (2009). Cognitive functioning in major depression–a summary. Front. Hum. Neurosci. 3, 26.
16. Hattar, S., Liao, H.W., Takao, M., Berson, D.M., and Yau, K.W. (2002). Melanopsin-containing retinal ganglion cells: architecture, projections, and intrinsic photosensitivity. Science 295, 1065–1070.
17. https://www.frontiersin.org/articles/10.3389/fpsyt.2019.00100/full
18. https://onlinelibrary.wiley.com/doi/10.1111/jnc.15356?af=R