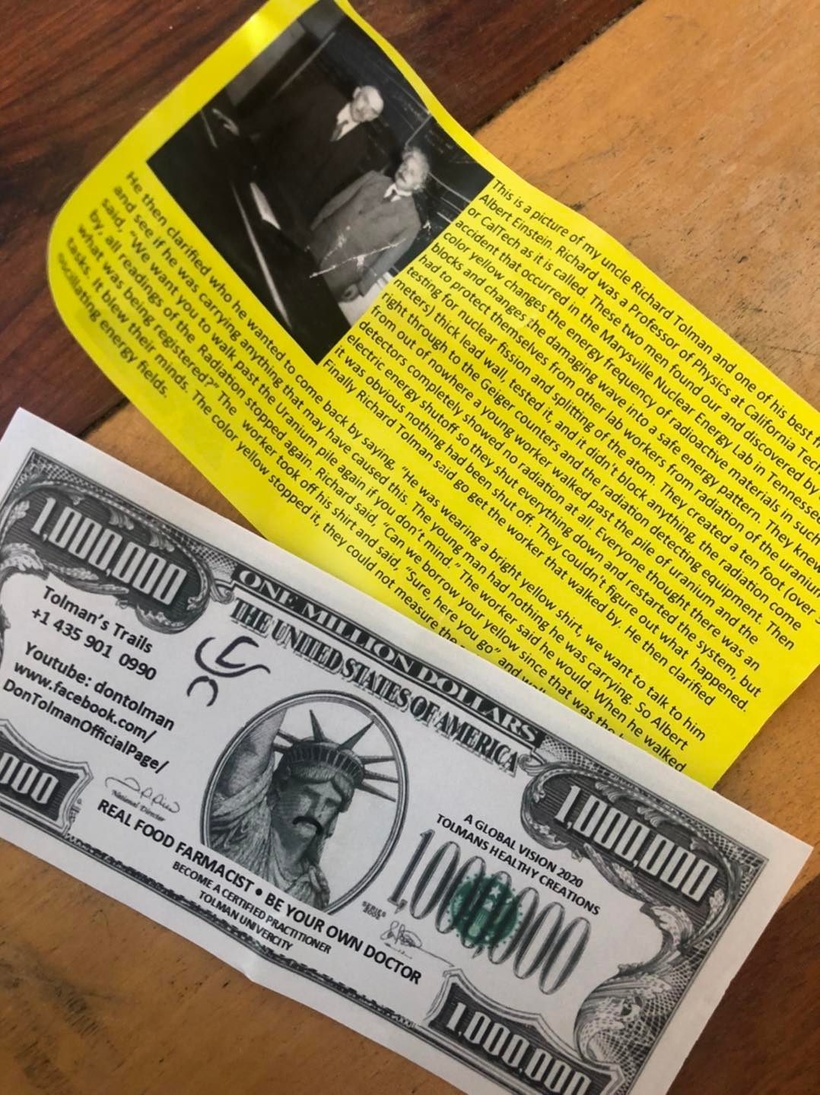
For a long time, there has been a guy running around the world advocating wearing yellow clothing to block radiation. Is this pseudoscience or might there be something to this? You might even run across this pamphlet from time to time.
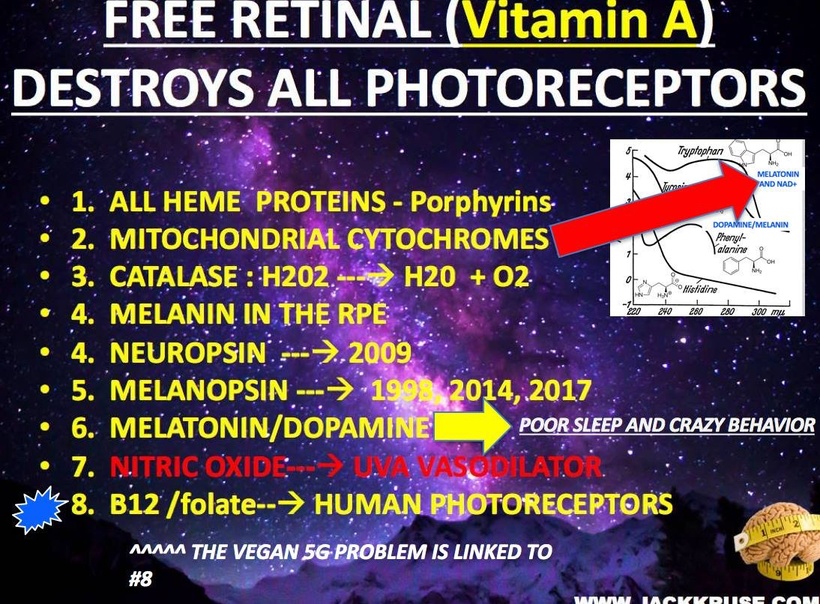
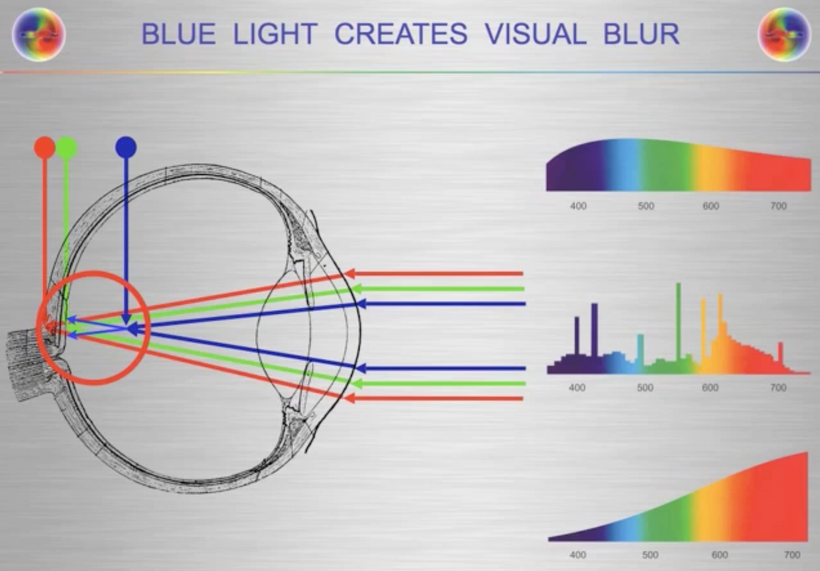
What is a possible mechanism for this observation in Nature? Many people do not know when I look into the eye of a patient with an ophthalmoscope one of the things I am looking at is the macula lutea. The macula contains the fovea where color vision is the sharpest. “Lutea” is yellow in Latin. This area collects yellow carotenoids to decrease the visual blur that is induced by blue light because blue light is the high frequency of light and it is the frequency that bends the most for the macula to handle. Yellow is the complementary color of blue.
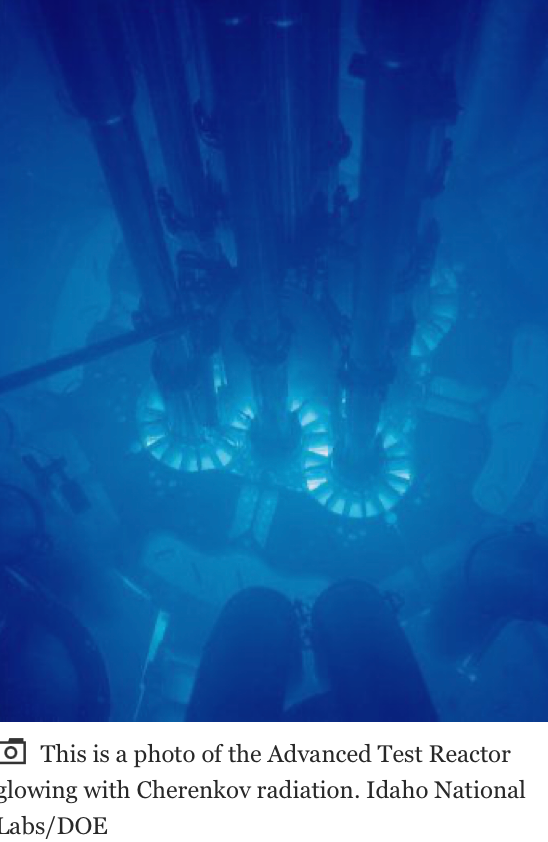
In nuclear reactors, the heavy water that contains spent fuels emits Cherenkov radiation. The frequency spectrum of Cherenkov radiation by a particle is given by the Frank–Tamm formula. Unlike fluorescence or emission spectra that have characteristic spectral peaks, Cherenkov radiation is continuous. Around the visible spectrum, the relative intensity per unit frequency is approximately proportional to the frequency. That is, higher frequencies (shorter wavelengths) are more intense in Cherenkov radiation. This is why visible Cherenkov radiation is observed to be brilliant blue. Cherenkov radiation is a form of energy that we can perceive as a blue glow emitted when the electrically charged particles that compose atoms (i.e. electrons and protons) are moving at speeds faster than that of light in a specific medium. Ironically, most Cherenkov radiation is in the ultraviolet spectrum—it is only with sufficiently accelerated charges that it even becomes visible to our retina; the sensitivity of the human eye peaks at green, and is very low in the violet portion of the spectrum. This helps explain this scientifically. Anyone who calls it pseudoscience without examining it for themselves should not be listened to.
HERE IS WHAT THE RADIATION LOOKS LIKE INSIDE A NUCLEAR REACTOR
DOES SCIENCE PROVIDE A POSSIBLE ANSWER FOR THIS OBSERVATION IN NATURE?
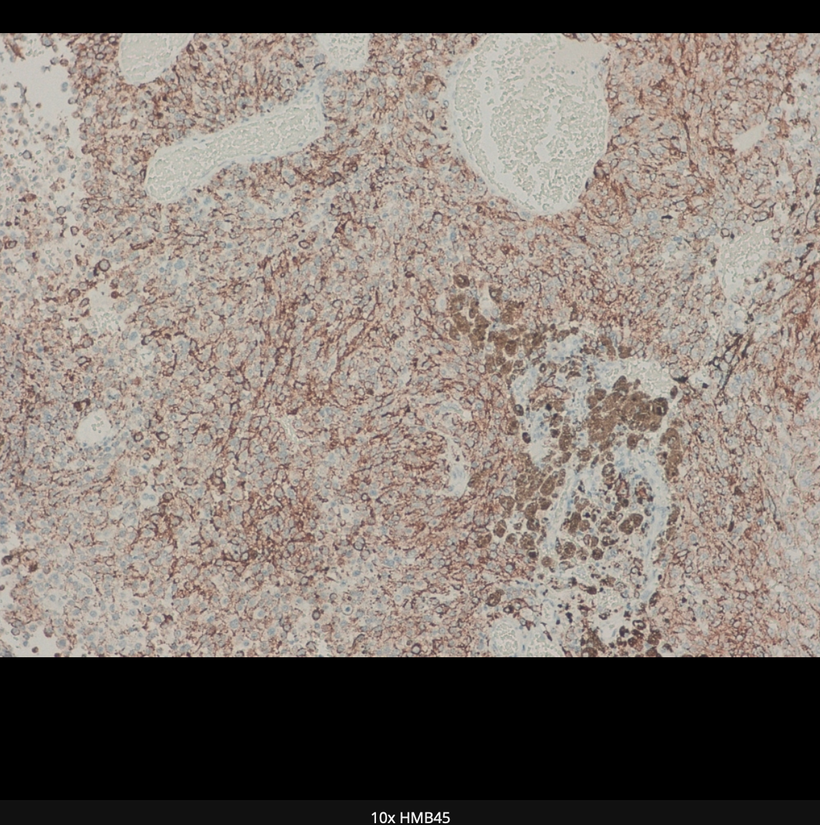
Can Gold be used as nnEMF radiation shield for melanin protection?
Now for more science related to this idea.
In 1988, this was published in the NY Times and I remembered reading it. Remember gold emits a yellow color because of Einstein’s relativity equations.

What was in the article I read in 1988 in New York City?
I was dental school in 1988 and I was learning about class 5 gold foil dental reconstructions and came across this article back then.
GOLD, one of the heaviest chemical elements, is the basis of a new lightweight plastic foam under development as a radiation shield.
Scientists at Texas A&M University have found a way to intersperse gold atoms with other atoms in the long molecular chains that make up polymers. By bubbling gas through the gold polymer, it can be expanded into a light foam that reportedly shows great promise as a shielding agent against neutrons and other types of radiation.
Dr. John Fackler, director of the program, said the new polymer combines gold with triphenylphosphine, a compound of carbon, hydrogen, and phosphorus, in a form that may be suitable for making anti-radiation garments.
The polymer is 11 percent gold by weight, and the gold atoms in the substance efficiently scatter or absorb most forms of radiation, including X-rays. Chemically incorporated into a polymer, gold is less poisonous than other heavy metals that also block radiation.
Metallic gold is not poisonous, but when incorporated into compounds it may be. Dr. Fackler said that because gold is chemically very stable, it tends to revert to its native state from some of the compounds it forms. ”We often have trouble with shiny, yellow metallic gold precipitating out of liquid compounds – just what refiners want, but the opposite of what we want,” he said.
The gold polymer the Texas group has developed looks like plain white plastic, Dr. Fackler said, but it emits a yellowish glow when exposed to ultraviolet light.
SUMMARY
Many might find this shocking but there is a lot of science behind these claims about the color yellow and the atom of gold. One of my former members in the mining industry could not believe this when I share it with him during a consult I did on him in 2015 about his melanoma risk.
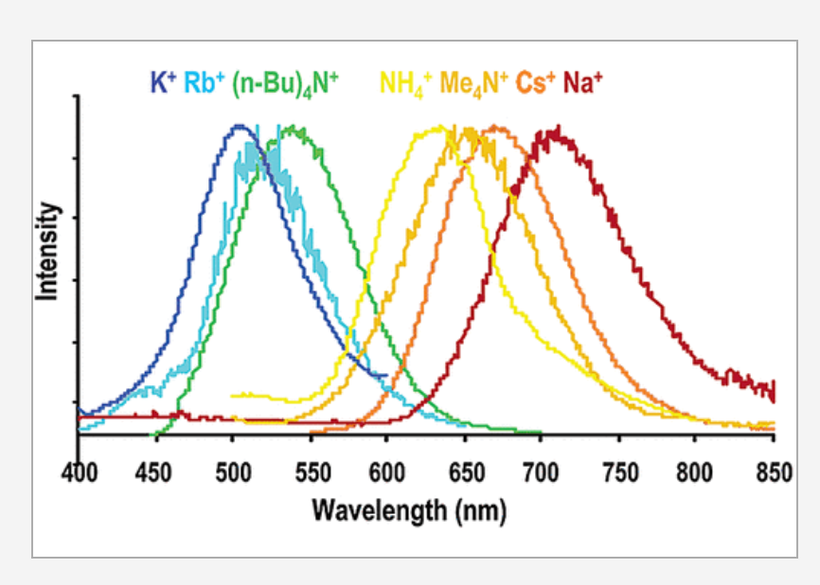
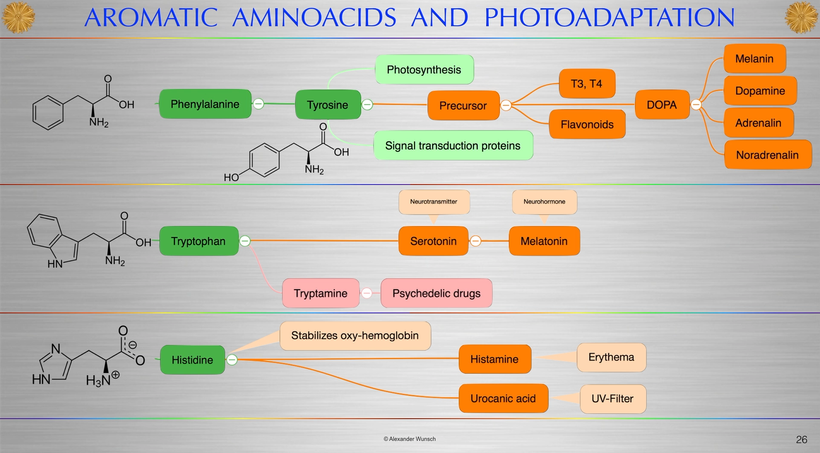
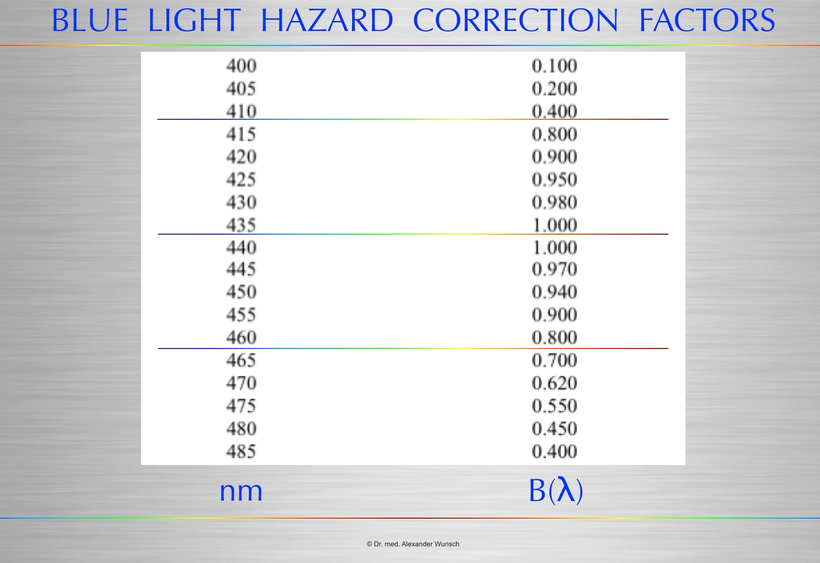
Above you see a series of bis(thiocyanato)gold(I) complexes with Au−Au interactions show luminescence in the range from 500 to 670 nm. These frequencies include the blue light frequencies that cause the blue light hazard in the human retina. This picture below from Alexander Wunsch, MD show this effect.
The series of salts correlates emission energy with the reciprocal of the Au−Au distance. As the Au−Au distance increases, the emission energy decreases. The ligand system provides no framework for the Au−Au interaction. The emission energy seems totally determined by the Au−Au distance.
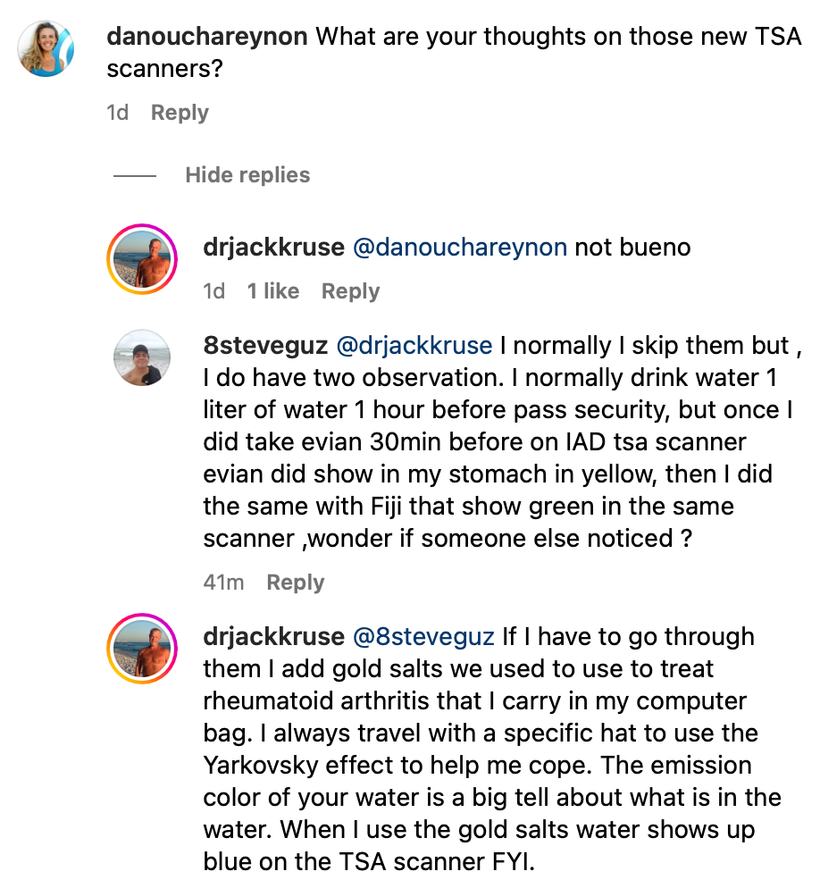
So when I am in a country where I cannot opt out of the new TSA scanners I reach into my computer bag to protect melanin in body. I usually take it 30 minutes before flight. Last time I had to do this was in Germany when I went to speak at Flowfest. I posted about this hack on Instagram.
Gold therapy, while not commonly used in the treatment of RA today, is still available in oral capsule form as Ridaura (auranofin). The injectable forms—Myochrysine (aurothiomalate) and Solganal (aurothioglucose)—are no longer manufactured but they can be compounded by a pharmacy. Below is my travel jacket I wore to Europe the last time I went there. The jacket is definitely not a fashion statment.

Jason Bowden Smith, a former entrepeneur member who was a mining industry executive, was with me in Mexico 4 months before the Germany talk and I told him about the jacket hacks and the gold hack and why I was doing it to go to Europe. Here is the picture taken that morning at 8:34 AM on January 4, 2018. He just did not believe what I shared with him. That maybe explains why reality unfolded as it did.

The gold salts and clothing are expensive hacks to protect melanin, but I think my health is worth the expense. I first mentioned this effect to Jason Bowden Smith in a consult in 2016. He was from Australia and had a very challenging medical history. We did a few consults when he was alive & during a consult I told him about these effects for long flights to mitigate TSA scanners, cosmic/gamma radiation exposure, and WiFi toxicity from passenger use around him.
Gold therapy can induce an internal Yarkovsky effect (below) for melanin protection. People who have had melanoma and who still are afraid of the sun should be told about this mitohack. Very few of my clients needed this. Unfortunately he did need the advice and he got it. UInfortunately, he believed a lot of the propaganda that is floating around in Australia even today about the sun.
Jason took a lot of circumpolar flights in his life. I thought this was linked to his REAL melanoma & thyroid risk and I told him about POMC and melanin. I told him a lot of what you’re learning now in this blog series a long time ago. In fact, Jason was with me in a meeting the night before my clinic opened in New Orleans in December 2018 to talk about a business opportunity about this very topic since he had deep connections with gold miners in Australia. My nurse, Chantal was present at this meeting.
Anyone who was with me in Germany knows I did not feel well when I was in Germany because they had recently turned on 5G in the city I was speaking in. I distinctly remember Jason mocking me before my talk when I took my clothes off and laid in the sun to get ready to speak. He kind of pissed off my nurse who was with me at the event. He just did not believe that something on the surface could have that big an effect on our mitochondria below. I told him that the gold/yellow can protect quantum coherent process happening with 1/2 nuclei spin magnetic moments in our colony of mitochondria to maintain quantum coherence. I told him everything that is important in quantum biology happens on the surface before it changes the matter inside of us. I told him that in June of 2018 I was goning to unleash this in Vermont. I did. Here is the slide from that event.
I spoke in Germany right after the Vermont event on July 6th, 2019. Something else happened at that talk that others can verify. The meeting organizer subtracted 45 minutes from my talk and only gave me 15 minutes to speak. Matt Maruca and Jason were both there also as a speaker and they saw this go down. He made me a bet that there was no way I could do a nnEMF talk for the German biohacking community in the 15 minutes. I went and powered up in the sun, drank one liter of DDW, and laid shirtless for two hours before my talk and missed many talks doing so. Matt then got a red LED stop clock and put it in his lap to show me my time to see if I could do it. Notice the first slide in the talk.

I finished the talk at 14:59 and everyone who was at the event was astounded I got the talk done in such a short time frame. The talk was so good that the Q & A lasted two hours outside the event when I was ushered off the property because the event was closing. Jason Bowden Smith spent that two hours in the sandpit of the event with me trying to ask me more about this science. It was the last time we met live in person and we never spoke about it again. He died soon after it. I feel that he never called me back to speak about things because he felt foolish that he had an answer from 2016 and thought it was a joke. Generally I don’t joke around on consults. I am all business.
Below this was me in Germany live on the stage during the Q&A before it spilled outside. That jacket was tailored to be infused with gold microfiber threads hidden in the silver etchings, hence the reason I bought it and wore it. I still have this jacket today.

What is the Yarkovsky effect?
The Yarkovsky effect is defined as a thermal radiation force that causes objects to undergo semi-major axis drift as a function of their size, orbit, and the COLOR of the material properties in the matter that makes up the object in question.
Melanin has a massive Yarkovsky effect inside of cells because of its color. so anything you can do to reflect and deflect incoming radiation should help protecrt you melanin sheets.
The Yarkovsky effect is hard to predict, though. Scientists have to know the asteroid’s mass, size, and shape. They also need to know the patterns of light and dark on its surface, because lighter colors reflect more sunlight, while darker colors absorb more.
The best measurement of the Yarkovsky effect so far is on an asteroid named Bennu. The effect has altered Bennu’s position by about a hundred miles in just a dozen years. So when you hear something that sounds ludicrous. Remember it is the height of ignorance to say it is pseudoscientific without looking deeper at the issue before making a decision.
Just because something’s logical, doesn’t mean it’s not wise. Something can make sense in and of itself, but when tested against reality yield an undesirable or inefficient outcome. Being seduced by impractical logic is antithetical to wisdom, you just feel smart despite being wrong. Sometimes chosing comfort over wisdom might kill you.
CITES
2. A version of this article appears in print on Sept. 6, 1988, Section C, Page 11 of the National edition with the headline: SCIENCE WATCH; Gold as Radiation
3. https://pubs.acs.org/doi/pdf/10.1021/ja00310a028
4. https://www.instagram.com/p/CsJcPQUM2a9/
5. https://forum.jackkruse.com/threads/dog-health.27663/#post-321327