I have been asked by many of you to give you my best guesstimate of what to do when you are vaccinated or injured. The same thing is true about long COVID. Contained in the next few blogs in the CPC series will give you my current state of thinking.
Just some random thoughts on all mitochondrial diseases and mRNA vaccine damage.
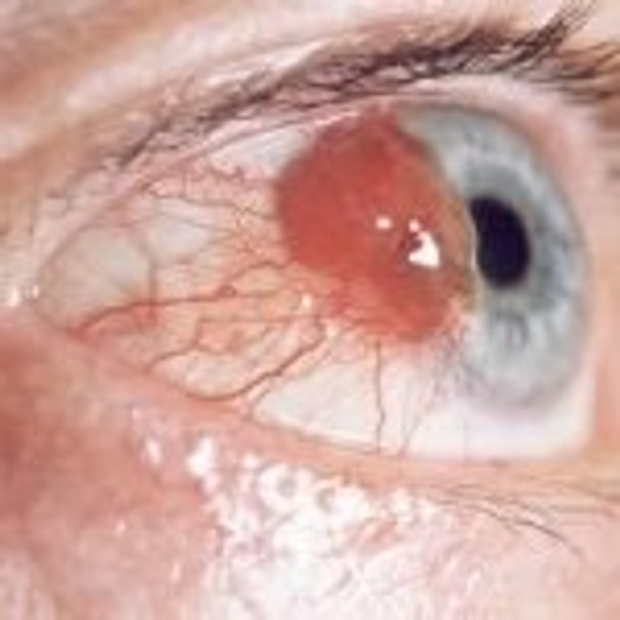
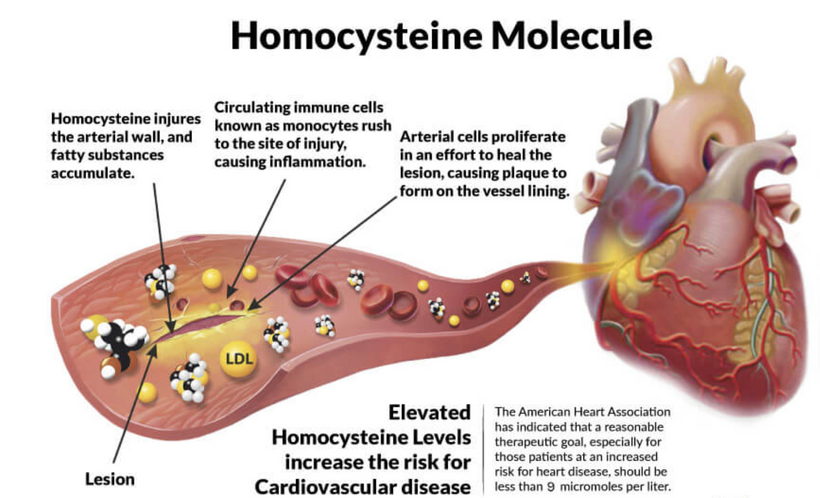
Intravascular injection of these jabs appears to cause a problem in the coronary and brain circulation which leads to acute elevation of homocysteine.
The brain is exposed to most of the constituents of plasma including homocysteine as a result of the disruption of the blood-brain barrier after stroke, head trauma, and stress. I believe the mRNA jab causes the same physiologic response in blood vessels. The question, therefore, arises as to whether or not homocysteine is able to selectively stimulate the release of excitatory amino acids in COVID illness.
Homocysteine has been under a lot of speculation since its discovery in 1932. Its chemical properties showed a similarity to cysteine, hence the name homocysteine. The heating of the amino acid methionine with sulphuric acid led to this amino acid of interest. The importance of this discovery cannot be emphasized without alluding to the 1955 Nobel Prize in Chemistry, awarded to Vincent du Vigneaud on for his work on biochemically important sulfur compounds.
As homocysteine rises so does IL-6. Homocysteine induced mRNA expression of the pro-inflammatory cytokines called monocyte chemoattractant protein-1 (MCP-1) and interleukins involved in the cytokine storm. IL-6 is one such chemical.
IL-6 is linked to just about every mitochondrial disease on this planet. IL-6 destroys the redox potential everywhere it is found because it raises cortisol in the stroma of organs. When cortisol is high, collagen is destroyed, it loses its piezoelectric and flexoelectric signaling while and cells get larger in volume and mass. While this goes on simultaneously, homocysteine rises, Vitamin D lowers, and methylation becomes disrupted. Nitric oxide is destroyed and clotting becomes more likely.
Homocysteine is a key determinant of the methylation cycle’s ability to operate in blood vessels.
I bet that people like Whoopi Goldberg who got COVID twice after her jab have a very altered SAM-to-SAH ratio.

The SAM-to-SAH ratio defines the methylation potential of a cell and is a proxy for the redox potential in the circulatory system. How?
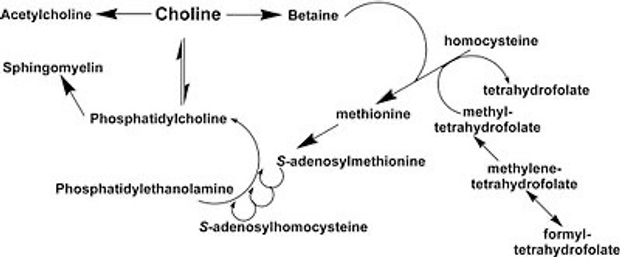
Condensation of methionine with ATP, leads to the formation of SAM (S- Adenosylmethionine). The methyl group attached to the tertiary sulfur of SAM can be transferred and therefore can cause methylation of other substances in the body that need it. It is a marker of how energy transfer is accomplished. This methylation is accompanied by energy loss, so this reaction is irreversible. The demethylation reaction leads to the formation of SAH (S- adenosylhomocysteine). SAH is a thioether (a sulfur bonded to two alkyl or aryl groups) analogous to methionine. Recall that methionine is the start amino acids signal in the creation of every human protein. The fidelity of this signal is highly leveraged to redox power in the cell.

Homocysteine is a key determinant of the methylation cycle and how easy energy is transferred from mitochondria to proteins in the body. Long COVID is likely related to high levels of homocysteine due to poor energy transfers. Homocysteine is methylated to methionine, which undergoes S-adenosylation and forms S-adenosylmethionine (SAM). S- adenosylmethionine is the principal methyl donor for all methylation reactions in cells.
High Homocysteine —> high Hageman Factor —-> increase platelet stickiness —> Clots
When homocysteine is elevated, water flows in cells are altered, and swelling ensues worsening the volumes and mass relationship. We saw this in lung edema in COVID ICU admissions and death. Any time these are altered apoptosis and autophagy programs are altered in the colony of our mitochondria. This is why water has its own specific nuclear footprint when we see cancer on an MRI. There are massive alterations to the Rayleigh Benard cycling of water inside cells. Everyone with sleep apnea (hypoxia) has high levels of IL-6 in the brain which alters the EZ of water in the brain. It correlates 98% of the time with low DHEA levels. This tells us cortisol is being shunted over the sex steroid hormones in response to the homocysteine elevation. This is known as prenenolone steal syndrome. COVID is a known hypoxia-related disease associated with acute spikes in homocysteine.
This is why DHEA and sleep are linked for the clinician. We can tolerate more inflammation within our brain from a ketogenic diet because our immune system is getting more electrons. Ketogenic diets are all about deuterium depletion of the mitochondrial matrix that improves piezoelectric ability. Ketogenic diets also restore NAD+ by producing more NAD+.
What most don’t know is NAD+ has two roles in biology– the common one as a cofactor vs the uncommon role as a signaling molecule. NAD+ does two things: it serves as a cofactor in redox and important metabolic reactions in which case it is shuttled back and forth between the NAD+ and NADH forms but is not consumed, and number 2, it serves as a signaling molecule in which case it is consumed as a substrate by sirtuins. Of the two roles, biology only talks about the redox action, when health and longevity are controlled with NAD+ is consumed by sirtuins.
NAD+ levels are a proxy for the redox state.
I have noticed that everyone who gets the mRNA jabs are losing their redox power to some degree because their homocysteine levels seem to rise just after the jab along with the HS CRP. The most common pathway they exhibit is a rising HS CRP, falling Vitamin D level, and a problem with their SAM-to-SAH ratio. Hyperhomocysteinemic (HC) states tend to decrease this ratio, leading to decreased methylation potential. The acute rise in HC seems to define an acute failure of the methylation potential of a cell after the jab. As homocysteine levels rise so does the risk of myocarditis.
There is some evidence that indicates that homocysteine can lead to global DNA hypomethylation and DNA damage. It may also suppress transcription of cyclin A in endothelial cells all associated with oxidative stress.
Several studies demonstrated that homocysteine is capable of triggering neuronal damage via oxidative stress, DNA damage and activation of pro-apoptotic factors in mitochondria in cell cultures or animal models.
Cell exposure to homocysteine seems to lead to a significant reduction of cell viability. The length of time homocysteine seems to affect cell viability and how it sensitizes them to ROS. Cell exposure to homocysteine for a period of 3 days did not induce any significant change in Reactive Oxygen Species (ROS) levels, but incubation with homocysteine for 5 days resulted in a 4.4-fold increase in ROS production.
We know from Comet assay tests that elevated homocysteine can triggered significant levels of genotoxic stress by seeing DNA fragmentation.
Bax and Bcl-2 mRNA levels in cells showed an increase by two-fold and 14-fold, respectively, in the case of 5 days exposure to homocysteine.
A time-dependent effect of homocysteine was also evident on the mRNA of chemicals involved in creating inflammation. The mRNA levels for the cyclins D1, E1, and A1 were increased by two-fold, six-fold, and five-fold, respectively, in cells exposed to homocysteine for 3 days. I think the virus and the jab elevate these things to cause adverse events.
In normal situations, the mRNA levels of all cyclins returned to the basal levels after 5 days of incubation with homocysteine. I do not believe this is true in people who get the jab. I think the mRNA of the spike proteins has far too much durability and this leads to the chronic elevation of the cyclins D1, E1, and A1. I believe this is driving the cases of myocarditis in the yound people. Normally, there is no chronic immune deposition of mRNA, but with these injections we know the mRNA is staying around way too long in T cells and monocytes. (see pic above for meaning)
WHAT SHOULD PHYSICIANS CONSIDER NOW?
If I was running the US response, I would do a few things.
First, I would be making physicians order levels of p21 in vaccine injured people.
P21 has been found to promote cell cycle arrest following activation from various stimuli. It is known to inhibit the cell cycle progression, leading to cell cycle arrest. A major cause of p21 activation leading to this outcome is the presence of damaging agents such as the mRNA spike protein from the vaccine.
The protein p21 (also known as WAF1, CIP1 or SD11) regulates cell proliferation by inhibiting the cell cycle through the cyclin kinase pathway. It also has been shown to inhibit apoptosis induced by numerous stimuli.
The protein p21 is another key protein regulator of DNA damage induced cell death. In research it has been noted to be elevated via incubation with high levels of homocysteine. The longer homocysteine stays elevated the more dramatic p21 up-regulation and protein synthesis seems to occur.
What else can physicians do?
Second, I would look in their CSF with a lumbar puncture.
The brain has a limited capacity for homocysteine metabolism. Because of this it might makes analysis of the CSF helpful in injured patients.
There is some evidence that indicates that homocysteine can lead to global DNA hypomethylation and DNA damage. It may also suppress transcription of cyclin A in endothelial cells all associated with oxidative stress.
Several studies demonstrated that homocysteine is capable of triggering neuronal damage via oxidative stress, DNA damage and activation of pro-apoptotic factors in mitochondria in cell cultures or animal models.
Cell exposure to homocysteine seems to lead to a significant reduction of cell viability. The length of time homocysteine seems to affect cell viability and how it sensitizes them to ROS. Cell exposure to homocysteine for a period of 3 days did not induce any significant change in Reactive Oxygen Species (ROS) levels, but incubation with homocysteine for 5 days resulted in a 4.4-fold increase in ROS production.
We know from Comet assay tests that elevated homocysteine can triggered significant levels of genotoxic stress by seeing DNA fragmentation.
Bax and Bcl-2 mRNA levels in cells showed an increase by two-fold and 14-fold, respectively, in the case of 5 days exposure to homocysteine.
A time-dependent effect of homocysteine was also evident on the mRNA of chemicals involved in creating inflammation. The mRNA levels for the cyclins D1, E1, and A1 were increased by two-fold, six-fold, and five-fold, respectively, in cells exposed to homocysteine for 3 days. I think the virus and the jab elevate these things to cause adverse events.
In normal situations, the mRNA levels of all cyclins returned to the basal levels after 5 days of incubation with homocysteine. I do not believe this is true in people who get the jab. I think the mRNA of the spike proteins has far too much durability and this leads to the chronic elevation of the cyclins D1, E1, and A1. I believe this is driving the cases of myocarditis in the yound people. Normally, there is no chronic immune deposition of mRNA, but with these injections we know the mRNA is staying around way too long in T cells and monocytes. (see pic above for meaning)
WHAT SHOULD PHYSICIANS CONSIDER NOW?
If I was running the US response, I would do a few things.
First, I would be making physicians order levels of p21 in vaccine injured people.
P21 has been found to promote cell cycle arrest following activation from various stimuli. It is known to inhibit the cell cycle progression, leading to cell cycle arrest. A major cause of p21 activation leading to this outcome is the presence of damaging agents such as the mRNA spike protein from the vaccine.
The protein p21 (also known as WAF1, CIP1 or SD11) regulates cell proliferation by inhibiting the cell cycle through the cyclin kinase pathway. It also has been shown to inhibit apoptosis induced by numerous stimuli.
The protein p21 is another key protein regulator of DNA damage induced cell death. In research it has been noted to be elevated via incubation with high levels of homocysteine. The longer homocysteine stays elevated the more dramatic p21 up-regulation and protein synthesis seems to occur.
What else can physicians do?
Second, I would look in their CSF with a lumbar puncture.
The brain has a limited capacity for homocysteine metabolism. Because of this it might makes analysis of the CSF helpful in injured patients.
Third, I would assess plasma, urine, and CSF folate and vitamin B12 levels. I also would check each injured person for MTHFR C677T (methylenetetrahydrofolate reductase) polymorphism.
By adulthood, the folate related enzymes involved in purine and pyrimidine synthesis, decline almost tenfold. Folate plays an important role in the brain so a crucial mechanism is in play to protect the brain from folate deficiency. The level of 5 tetrahydrofolate in the cerebrospinal fluid is 3 times that of the plasma level and there exists an active process to maintain it. We should be checking these levels in cases who deserve it. Methionine synthase is the only enzyme in the brain (neural tissue) that is capable of converting homocysteine to methionine. Cobalamin (B12) is a cofactor hence making it essential to the brain. Most people with long COVID have significant problems with these assays in my opinion. We need to be asking better questions.
SUMMARY
Implementation is a process of putting into action what is necessary to achieve a desired outcome. It also involves follow-up to ensure objectives are being met. A good idea or resolution is not enough. It must be implemented and then executed. Beginning to act, starting to take small steps to consistently fall forward, while being persistence makes all the difference in our life’s. With all the things going on with COVID we have to do more to help those with injury. Ideation without execution leads to deletion of our resolutions.
Become aware of the high cost of bad medicine. In biology we often get what we deserve. Our actions have covert direct effects that our eyes are blind too and this blind-spot allows us to slip away from the policy of truth in policies being mandated today. Today, stick to a strict diet of inspiring books, podcasts, beautiful spaces with amazing sites and people capable of elevating you to a plane of rare air.
There are no absolute truths with COVID…………there are just facts that change on a time continuum. As time evolves, facts change and what was controversial now becomes reality.
Part two of this blog will be up next.
CITES:
1. Hankey GJ, Eikelboom JW. Homocysteine and vascular disease. Lancet. 1999;354:407–13. doi: 10.1016/S0140-6736(98)11058-9. [PubMed] [CrossRef] [Google Scholar]
2. Loscalzo J, Handy DE. Epigenetic modifications: basic mechanisms and role in cardiovascular disease (2013 Grover Conference Series) Pulm Circ. 2014;4(2):169–74. doi: 10.1086/675979. [PMC free article][PubMed] [CrossRef] [Google Scholar]
3. Harvey RA, Ferrier DR. In: Lippincott’s Illustrated Reviews, Biochemistry. 5. Rhyner S, editor. Philadelphia: Wolters Kluwer Health; 2011. pp. 264–5. [Google Scholar]
4. Guo H, Chi J, Xing Y, Wang P. Influence of folic acid on plasma homocysteine levels & arterial endothelial function in patients with unstable angina. Indian J Med Res. 2009;129(3):279–84. [PubMed] [Google Scholar]
5. Baszczuk A, Kopczynski Z. Hyperhomocysteinemia in patients with cardiovascular disease [Abstract] Postepy Hig Med Dosw. 2014;68:579. doi: 10.5604/17322693.1102340. [PubMed] [CrossRef] [Google Scholar]
6. Curro M, Gugliandolo A, Gangemi C, Risitano R, Ientile R, Caccamo D. Toxic effects of mildly elevated homocysteine concentrations in neuronal-like cells. Neurochem Res. 2014;39:1485–95. doi: 10.1007/s11064-014-1338-7. [PubMed] [CrossRef] [Google Scholar]
7. Shenov V, Mehendale V, Prabhu K, Shetty R, Rao P. Correlation of serum homocysteine levels with the severity of coronary artery disease. Ind J Clin Biochem. 2014;29(3):339–44. doi: 10.1007/s12291-013-0373-5. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
8. Carmel R, Jacobsen DW. In: Homocysteine in health and disease. Carmel R, Jacobsen DW, editors. Cambridge: Cambridge UP; 2001. pp. 183–93. [Google Scholar]
9. Wuerthele SE, Yasuda RP, Freed WJ, Hoffer BJ. The effect of local application of homocysteine on neuronal activity in the central nervous system of the rat. Life Sci. 1982;31:2683–91. doi: 10.1016/0024-3205(82)90712-3