Going forward over the next 3-5 years, I still expect many currencies including the dollar to continue to devalue vs hard assets (BTC), and for the dollar to probably be among the weaker major currencies during that timeframe.
I just finished my Q & A for members and laid out the case for the super cycle coming in the next few months. I know this was complex but the video above is a parody of what I told my tribe. Many people are not ready for what is coming. It is coming faster than the market and the public expect and the market is calling the bluff of Central Bankers world wide.
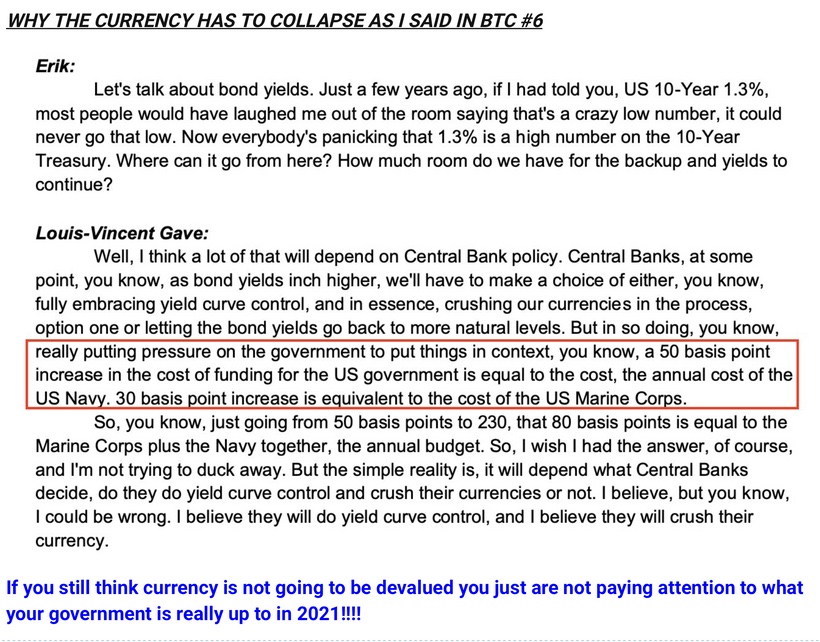
As the ten yield yield rises the Central Bank has one card to play. They will have to peg the short term bonds yield to stop the rising cost of government. In this environment commodity prices are going to spike. Growth Stocks will decline, and the currency will be under attack and the it will end in a devaluation.
We may be at the beginning of that edge right now.
Assets like Bitcoin in this environment will act like a basket ball underwater. The rapid rising of the ten year bond yield pushed Bitcoin down 30% but that fall is exogenous to the halving cycle. This means there is a huge potential energy bounce coming soon.
Eating Our Own Cooking = the collapse of fiat is real
The market has responded to the Central Bank actions and will force it to make a decision. The Fed is creating debt and now buying its own debt. Since Central banks are the biggest buyer in the market they can control price. They can surpress yields and if they fail, they can revert back to 1942-1951and put a permanent peg on the short end of the yield curve to make financing the government bills cheaper. The Treasury did this to pay for the WW2. The tradeoff here is that it destroys your currency. In 1950 the US had no debt so doing this had only one bad outcome: High inflation that would slow the economy. At the end of Truman second term his efforts were destroyed by the Fed’s peg rate.
With today’s debt rates the risk is complete hyperinfation and eventual currency devaluation in rapid fashion. I believe we are at that edge right now.
Based on the action of the VIX I believe most of Wall Street is unaware how close to the edge we really right now.
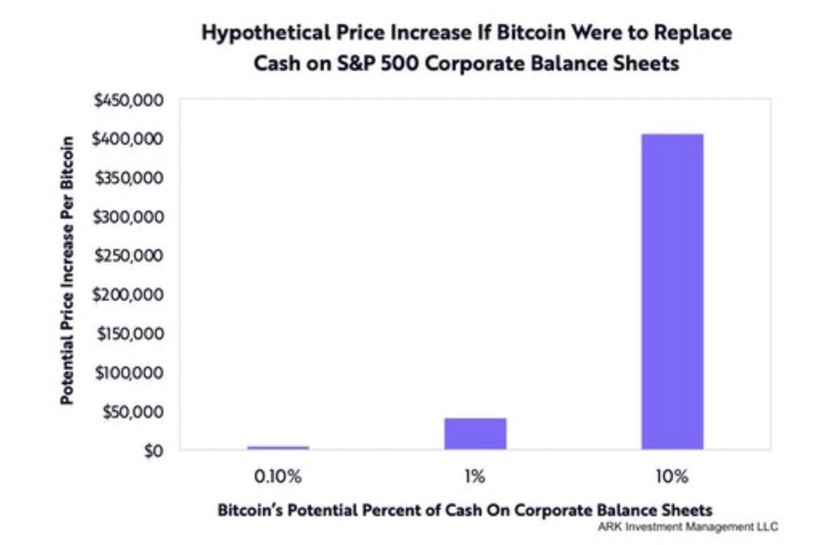
As bond yields in the 10 year go higher government funding cost become explosive and they lose control of the balance sheet rapidly. If the Fed pegs bond rates scarce assets will soar high. Example is below.
The choice of the Fed will make is going to play out by summer. Congress is adding fuel to this fire by passing a 1.9 Trillion stimulus bill that has no COVID relief. This money printing will push the dollar lower. I see the perfect storm brewing.
If the currencies collapses you can bet BTC will go up in parabolic fashion.
I hope you are all ready for this reality during the Ides of March.
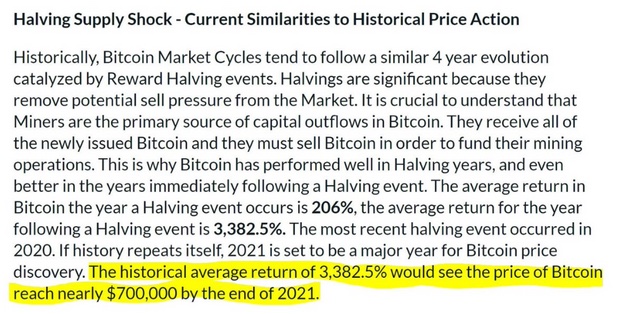
The halving cycles are associated with price dislocations. Generally the 18 months after a halving is when it is very bullish to own BTC to capture alpha on its price. Right now we are six months past that dislocation. The price movement from Feb to October 2021 is predicted by many models to be staggering. The stock to flow model is the one most cited on the internet seen below.
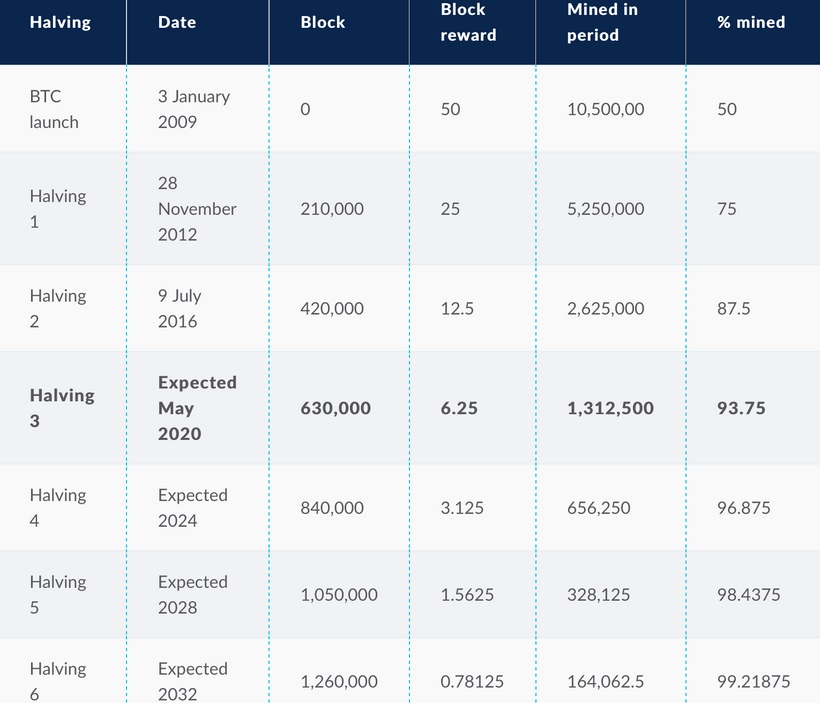
The halving process reduces the future supply of bitcoin by 50% for the next 210,000 blocks, when this process will repeat again. If demand stays constant, and this factor is not already priced into the market value of bitcoin, the value of bitcoin would rise. However, it is increasingly difficult to determine the intrinsic value of bitcoin due to its complexity.
The third halving was marked when the 630,000th block was mined. This bitcoin halving will see the mining reward drop from 12.5 bitcoins per block to 6.25 bitcoins. At the end of this halving 93.75% of all Bitcoins will be in existence. Right now 61% of Bitcoin has not moved in over a year. This tells us in this halving we are in now that supply is being constricted.
As you can see from the above table, the amount of bitcoin mined and the block reward drops by half at every halving event. By 2032, over 99% of bitcoin will have been mined and it is estimated to take up until 2140 until 100% of the total bitcoin is mined.
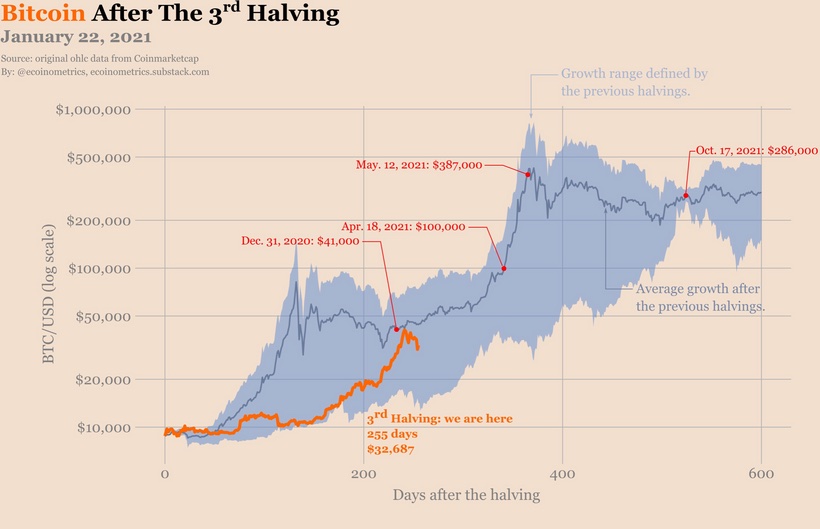
The ideal time to be in the BTC market is day 200-400 of the halving cycle. This is where parabolic growth appears to manifest. That time frame fluctuated based on some variables. Currently we are in that phase now in this halving cycle. This cycle however may not be like any other.
With halvings investors need to pay attention to key metrics. The key data points to watch leading up to the halving which include; countdown clocks, the overall hashrate, and the price per BTC and the bitcoin network difficulty rate. All of these determine when the next halving comes to the market. Right now that target looks to happen in April of 2024.
The hash rate for me, reminds me of the metabolic rate of the Bitcoin organism.
Observers can watch BTC’s price using markets.Bitcoin.com, as well as observe BTC’s network hashrate via charts.Bitcoin.com. Both of these resources are updated every day in real-time and people can observe the network difficulty as well. The data and analysis web portal Coin Dance,which covers all three Bitcoin-based branches (BTC, BCH, and BSV), is also a great resource to use if you are watching the network’s activities after the halving. Glassnode has all of this data as well.
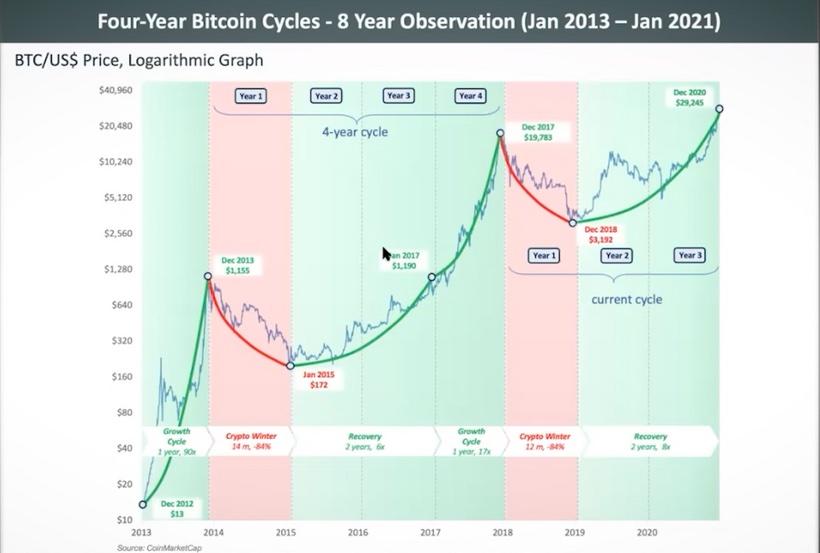
The first halving, which occurred in November of 2012, saw an increase from about $12 to nearly $1,150 within a year. The second Bitcoin halving occurred in July of 2016. The price at that halving was about $650 and by December 17th, 2017, Bitcoin’s price had soared to nearly $20,000. The price then fell over the course of a year from this peak down to around $3,200, a price nearly 400% higher than Its pre-halving price.
The mathematical theory of the halving and the chain reaction that it sets off works something like this:
The reward is halved → half the inflation → lower available supply → higher demand → higher price → miners incentive still remains, regardless of smaller rewards, as the value of Bitcoin is increased In the process.
In the event that a halving does not increase demand and price, then miners would have no incentive as the reward for completing transactions would be smaller and the value of Bitcoin would not be high enough. To prevent this, Bitcoin has a process to change the difficulty it takes to get mining rewards, or, in other words, the difficulty of mining a transaction. In the event that the reward has been halved and the value of Bitcoin has not increased, the difficulty of mining would be reduced to keep miners incentivized. This means that the quantity of Bitcoin released as a reward is still smaller but the difficulty of processing a transaction is reduced. All of this is built into the code of BTC blockchain. Satoshi was brilliant.
SUMMARY
The root problem with conventional currency is all the trust that’s required to make it work. The central bank must be trusted not to debase the currency, but the history of fiat currencies is full of breaches of that trust. Banks must be trusted to hold our money and transfer it electronically, but they lend it out in waves of credit bubbles with barely a fraction in reserve. We have to trust them with our privacy, trust them not to let identity thieves drain our accounts. In this Fourth Turning all trust is gone. We have Biden getting ready to print another 1.9 Trillion dollars.
The environment is changing now favoring Metcalfe law dynamics. As the number of users grows, the value per coin increases. It has the potential for a positive feedback loop; as users increase, the value goes up, which could attract more users to take advantage of the increasing value. This is especially evident with the actions of corporations like Micro$trategy this AM.
1. Bitcoin’s price appreciated +9881% overall after Halving #1.
2. Leading up to Halving #2, Bitcoin rallied 383% to reach the pre-Halving top of $794.91.Bitcoin rallied 4080% in 524 days to reach the Market Cycle top of $20,074.
3. After the 2018 Bear Market where price retraced -84.5%, Bitcoin bottomed at $3152, approximately 511 days before Halving #3. Leading up to Bitcoin’s third Halving, Bitcoin rallied +343% to reach the pre-Halving top of ~$13,900. Overall, Bitcoin has rallied +805% since its $3152 March 2020 bottom so far, eclipsing the previous All Time High of $20,000 in the process. Today, on Mardi Gras Day it is at its all time high above 50,000K
Bitcoin’s post-Halving #3 performance confirms an important, historically-recurring tendency across all Halvings:
1. The Bitcoin Halving serves as a major catalyst for new Bitcoin Bull Markets.
2. Several months after each Halving, Bitcoin tends to eclipse its old All Time High, rallying to new, uncharted price levels.
3. Most of the exponential growth in Bitcoin’s price as a result of the Halving tends to occur after the Halving
Let’s now focus specifically on Bitcoin’s performance after Halving #3:
Bitcoin is up +648% since its $8161 price point at the time of Halving #3. This number is lower than other cycles.
MY CAVEAT: Demand is already far surpassing the ability of miners to produce Bitcoin, and demand is rising exponentially. We found this out from the recent GBTC buys. The likelihood that we are entering a super cycle for the asset class is very likely. The 4 year cycle theory may no longer apply right now.
What defines a supercycle? Everything begins to accelerate at an incredible speed for the value of the king of digital currencies.
We must pay tribute to Michael J. Saylor for having had the audacity and intelligence to adopt this strategy since August 2020. He just borrowed another 900 million dollars for 0% interest and plans to buy BTC with it immediately. What do you think this does to the value here considering how the supply is narrowing?
Besides, Michael J. Saylor has become a formidable ambassador for Bitcoin. Rather than simply profiting from Bitcoin, Michael J. Saylor has decided to reveal his Bitcoin Playbook to as many people as possible. This will drive Metcalfe’s law in the Bitcoin ecosystem.
At a conference held in early February 2021 by MicroStrategy, Michael J. Saylor has answered the many questions that all the treasuries of major companies are asking themselves now. Elon Musk already bought 1.5 billion of Bitcoin as a result of Saylor’s idea being made public.
If we extrapolate Bitcoin’s post-Halving #1 performance to Bitcoin’s post-Halving #3 performance, Bitcoin could rally anything between +1742% and 2200%.
A +1742% rally after Halving #3 would result in a ~$150,000 Bitcoin.
A +2193% rally after Halving #3 would result in a ~$188,500 Bitcoin.
What if we extrapolated Bitcoin’s post-Halving #2 performance (+4080%) to Bitcoin’s potential post-Halving #3 price appreciation?
A +4080% rally after Halving #3 would result in a ~$342,000 Bitcoin.
This defines what the current super cycle might create for you Treasury. So if you think it is too early to buy at 51,000 dollars, you are not part of my tribe. You might be part of their tribe below.
Bitcoin bottomed 511 days prior to Halving #3.
Should Bitcoin rally for 511 days after Halving #3, that would mean that Bitcoin would peak in early October 2021. That means the run that is coming from February 2021 until November might blow your mind.
Once they understand the DNA of Bitcoin they will buy it in droves. I think that time is upon us.
The circadian biology of Bitcoin is found in its hash rate. A new Bitcoin block is found every 10 minutes, this genetic code enables Bitcoin’s cells to effectively communicate and coordinate with each other despite enormous distances. It is the internal clock that sets the metabolic rate of the Bitcoin organism. Hashrate has speed up in this cycle becoming an early indicator that this cycle is different.
The code of life is written into an organism at its inception. Satoshi carefully architected Bitcoin’s DNA, or genetic code, to be the best sound money ever created. We can think of Nakamoto’s white paper as Bitcoin’s DNA genetic code. It represents instructions that have been written to incentivize the organization and coordination of cellular function. When corporations understand what this code means to value they will act rationally.
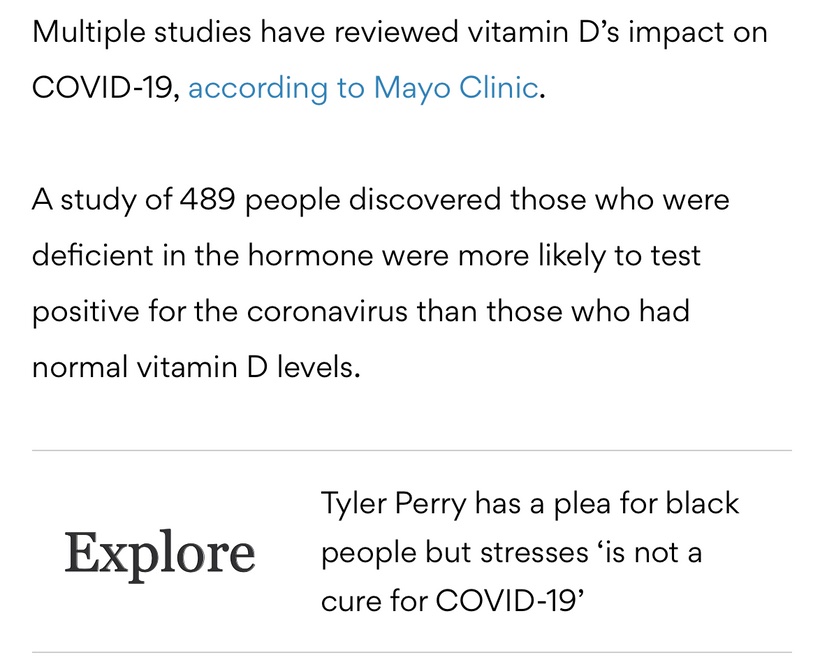
Why take an Rx blood thinner when the sun does it for free? Does this explain why darker skin people get COVID more, and get severe clotting issues with COVID, and die more frequently when they live at high latitudes and in cities where nnEMF and blue toxicity dominate? Can you explain this Uncle Jack? Look at the picture above and realize what is going on in blood when your skin is irradiated by terrestrial sunlight. Do you think the same waves are made in the blood when you are under fake light?
Do plants grow the same in the sun or with grow lights? Might this problem show up in us too?
Our modern lifestyle dehydrates us chronically and causes us to lose the ability to create Vitamin D and use magnesium in a proper thermodynamic way in cells. Both of these problems lead to clotting and a lack of immunity. It also is the reason why Cancer shows up in people who avoid the sun because of idiotic public health beliefs that the sun is toxic. This is our greatest risk factor for skin cancer in my opinion. Australia is the classic example of this modern risk factor today. Anyone who is struggling to get their Vitamin D levels higher likely has a co-morbid magnesium deficiency due to a lack of water from poor mitochondrial function at cytochrome C oxidase. People forget that one of the main by-products of mitochondrial energy transformation is the production is water at cytochrome C oxidase.
Many of these people dehydrate their colony of mitochondria when they live in an environment loaded with non-native EMF and blue light. What is the first thing that happens in the mitochondria when this occurs? It reduces the amount of melatonin the mitochondria make. This impairs both autophagy and apoptosis. When this happens neither change program is efficient at removing defective engines and disease present. That is Why COVID, CLOTTING, and CANCERS ARE all linked to a lack of sun and too much tech exposure.
Magnesium in a cell is a hydrophilic element on the periodic table, and without water, we lose intracellular Magnesium (Mg). 56 enzymes in mitochondria use Mg2+ as a cofactor. It turns out making melatonin is a Magnesium and water-dependent process. Making Vitamin D is also water and Mg dependent. There are 3 metabolic transactions from Cholesterol (Cholecalciferol) that occur under the surface of the skin where our “storage version” of Vitamin D (Calcidiol) is made. This 25(OH) version of D3 gets transformed in our kidneys and liver to the “active version” of Vitamin D (Calcitriol or 1,2,5 (OH) in the liver. All 3 reactions require Mg2+ as a cofactor. Mg, however, needs the mitochondria to make cell water in the cell to work properly. If the mitochondria do not make water, taking an Mg supplement is a waste of time and resources. It is physiologically impossible to have a 25(OH) blood test (“Storage-D”) to be less than 35 ng/dl and a Magnesium RBC level to be above 6.5mg/dL because of the negative feedback loops tied to calcium levels in our blood!
As a result, this is why melatonin levels are off in these patients. With time this ruins their sleep because melatonin forms another coupled cycle with cortisol and adenosine. This is why Magnesium and Vitamin D deficits walk together in mitochondrial damaged patients. This is why COVID people get the side effects they get. Some kids with COVID have enough redox power to avoid clotting but they get chronic fatigue instead. It will not change until their redox power is returned by changing the environment they are in. If this is allowed to persist chronically it is only a matter of time that clotting will occur or that will develop another chronic mitochondrial disease, like cancers. I think this is why Oz is loaded with melanoma.
If you want success in life, become a problem solver for your patients. Not a fixer.
Magnesium is also a co-factor for telomerase that controls our telomere lengths. When you marry this with a low melatonin level you begin to see why cancers will come as these people age. It is also the reason why dark people get the worse outcomes from COVID and why they COVID to begin with. Taking a vaccine won’t solve this problem but getting in the sun will. I also think people who use a ton of sunscreen are at risk for clotting, COVID, and chronic fatigue. What else exacerbates this linkage? A modern diet with undiagnosed high O6/O3 ratio due to seed oil usage with the use of carbohydrates out of season which also causes dehydration. One mole of fat creates 100-110 nmol of water. One mole of carbs produces 55 nmol of water in the mitochondria. Carbohydrates also contain more deuterium, and deuterium main function in the body when it gets into the mitochondrial matrix is to decrease the piezoelectric ability of the mitochondrial via the increased kinetic isotope effect. IT makes the mitochondria act more like a diamond, and less like quartz. A diamond carbon lattice is not compressible, while the SiO2 lattice of quartz is. This is why quartz is piezoelectric and why a diamond aren’t. This is why Nature only creates carbs in strong light cycles when the sun can offset the lack of metabolic water production from the sun in mitochondria at cytochrome c oxidase.
In medical school, I learned that Vitamin D was a hormone that was important in bone metabolism and that is where it really ended until I began to read about Vitamin D3 15 years ago. In all that published research, it uncovered what it really does for our cells. The major effect is that it modulates the immune system as its receptor is found on T helper cells (regulator cells), the same cells that are destroyed by COVID spike protein or how HIV infection wipes out in AIDS victims. So if your Vitamin D levels are low, FOR ANY REASON, they turn off the epigenetic switches on RNA/DNA/mtDNA genes that turn on the proper functioning of immune system protector cells to keeps us free of diseases from viruses, bacteria, mold, and fungal infections. In fact, since I got my level checked 15 years ago, I have not been seriously ill. The sun provides what we need. No mRNA can do this. When you give a person with low redox and a low D level an mRNA vaccine we should expect new variants of COVID that are more lethal. It appears our Public Health experts in the centralized medical systems did not expect this. My clients, in my decentralized practice, however, did.
SUMMARY
Artificial light creates a positive charge in most of the things in a cell. Galactic cosmic radiation also has positive nuclei and charge. These positive charges were accelerated in the shockwaves of supernovae throughout the galaxy and they randomly enter our solar system.
Redox power from the sun, manifests in living systems is all about optimizing the net negative charge in cells.
Its proxy is found in the charge carrying ability of water (dielectric potential) made in mitochondria which control intracellular endogenous glutathione levels. All things that cause inflammation carry a net positive charge. This is why pH matters in the care of COVID patients in a hospital. It predicts who is really in trouble.
If you need a clotting drug, you are, BY DEFINITION already blue light toxic, nnEMF overdosed, and get far too little sun on all parts of your body.
Creators are hard-driving, focused, dominant, independent risk-takers. Who are the emerging players on top of the Monopoly board in DeFi?
DeFi update Feb 5, 2021:
DeFi is becoming a cash flow machine. These protocols are generating annualized earnings (est.): Uniswap = $140M (60% of swaps) Aave = $100M (interest & flash loans) Sushi = $90M (15% of swaps) Maker = $45M (seniorage-based credit swap lines)
Most protocols are <2 years old. Ponder that.
We’re on the ground floor of incredible change that is on the way in DeFi!
The current DeFi narrative depends very heavily on the future of Ethereum. It is highly questionable now if it can ever evolve into a network, that has e.g. identity, governance, privacy, and scalability issues completely resolved in a manner, that’s required from a true financial services network. My bet is on something, where those four things are solved first.
I think paying attention to the volume of the coin of dollar business they do will give us clues who will crush it on ETH 2.0 monopoly board I spoke about earlier in this series. It will also tell us ETHER 2.0 is the real ground to rebuild the new monopoly board under DeFi financial services.
Genius isn’t necessarily coming up with everything from scratch, it’s knowing how to take some existing ideas and perceive them in a radically different way to come to a new way of thinking that can unlock value in something that’s very, very new. Your ability to critically think you must engage your imagination. This blog is about my synthesis of where the axis of value is being built on the Monopoly board. The true sign of wisdom is not the knowledge you acquire, it is how the data you feed into your brain is filtered through yourimagination to get to a place where you can see the results of innovation before anyone else does.
My top 5 crypto right now Feb 2021:
1. Bitcoin
2. Aave
3. Uma
4. YFI
5. ETH
I think 2, 3, 4 are the first pieces being added to the Monopoly board. I think they are lots on the board with foundations being poured now. It is early…..but what they do is all about how many of us are getting yield on our crypto accounts.
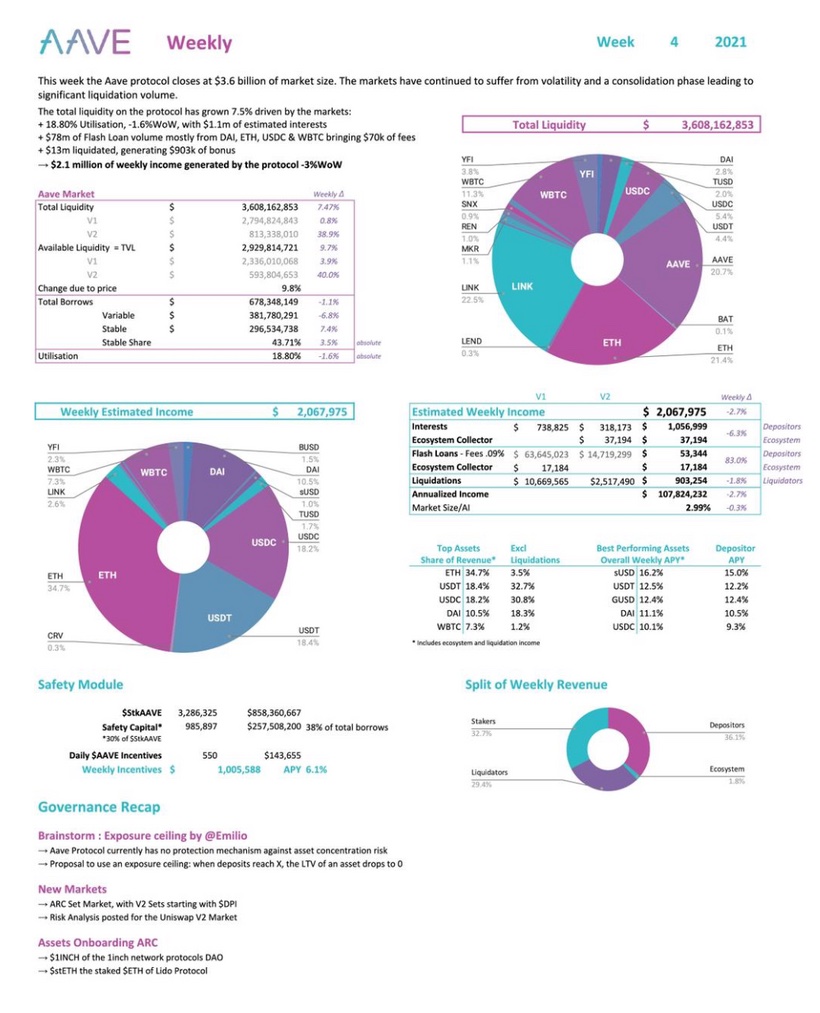
WHAT IS Aave?
For example, Aave is best described as a decentralized system of lending pools.
Users deposit funds they wish to lend on ETH2.0, which are then collected into a pool. Borrowers may then draw from those pools when they take out a loan. These tokens can be traded or transferred as a lender wishes.
To make it clear regarding revenues of ($aave): Estimated weekly Income : USD 2,067,975 Weekly incentives : USD 143,655 Yield APY : 6,1% Price to Sales : 67,5 x Volume/Market Cap : 19,58% DeFi is growing faster that anyone can imagine.
Why does AAVE have intrinsic value?
As the Patreon blog says, ETH 2.0 is not decentralized but Aave protocol is. That is why I think it becomes a key property on the monopoly board. AAVE plays a central role in the management of the Aave software, allowing users to vote on changes to its rules and policies.
Aave was released in mid-2020 and has went from 80-430 since I first bought it when I was in my last few days in Mexico in Dec 2020.
AAVE owner are able to vote on interest rates for certain loans and aspects of how deposits are managed. This makes it interesting to me. Interest is how banks operate. Aave is a replacement for bankers in the DeFi space. Aside from this utility, AAVE derives value from its finite supply, and the fact that it uses revenue from fees to buy AAVE and remove the cryptocurrency from circulation. This makes it decentralized.
Currently, 80% of fees collected by the Aave system are used to burn AAVE. THIS TELLS ME SUPPLY IS SHRINKING SO THE PRICE HAS TO GO HIGHER. I believe it might go higher than any other coin in 2021. The remainder is used to pay lenders in their space. The constant burning of AAVE is expected to reduce its supply, thus driving up the price of the token if demand remains constant. So far it has worked as I thought.
The 4 elements I have cited here (identity, governance, privacy, & scalability) are essential elements for a truly decentralized financial system. They are four legs of the DeFi table, if you don’t have one the system will eventually be out of balance and mean revert to the intrinsic value of the labor put into the code. For me, this is why I am not yet sold long term on ETH 2.0 as a chronic winner. I do think what is being built on it, may far surpass its value. I want to discuss how I see the “early axis of this monopoly board” is being built today in front of eyes.
Many don’t understand how projects using the Ethereum 2.0 protocol equates to higher Ethereum token prices, so here is how it happens. As the DeFi projects continue to go up like Aave, UMA, UNI, YFI it means ETH has to be used up to complete the transactions.
The way ETH 2.0 goes up is Gas. ETHER is the gas that makes the DeFi projects operate. So for a more accurate answer, I suggest doing some homegrown research.
My understanding is that actions taken on the Ethereum blockchain have operating costs per transaction. Right now early in the ETH 2.0 game gas is expensive. If you have to pay for the gas you hate this increased cost. If you do not, and just own ETHER you’ll love this because consumption of ETHER because it cuts supply and this eventually will drive the price. The problem is there is too much ETHER in the market now to drive huge price gains, but this is going to change over time and makes ETHER look like a great play ten years out in the way I view the market. Since ETH 2.0 just started in the last 6 months, gas is giving people sticker shock, but if you when you realize there are 37 billion money transactions already in DeFi projects you’ll begin to understand why this situation is something to pay attention to and understand clearly.
When you want to compute something on the blockchain, you have to pay for that privilege. That action can take the form of sending tokens from one ledger to another, or it can be the execution of a smart contract. That cost replaces the subtracted middlemen. This payment happens in something called Gas = ETHER. And Gas comes from ETH tokens. So any project on the ETH blockchain needs ETH to run. It burns Gas. Gas comes from ETH tokens. Every project on the ETH blockchain creates a demand for Gas, which creates a demand for ETH tokens. And this increase in demand leads to a higher token price. This is driving ETHER price movement now. This begs the question, if ETHER IS going to move, then what crypto assets are fueling this momentum?
UMA = the VIX
The Chicago Board of exchange (Cboe) Volatility Index, or VIX, is a real-time market index representing the market’s expectations for volatility over the coming 30 days. Investors use the VIX to measure the level of risk, fear, or stress in the market when making investment decisions.
For those of you who do not know what UMA does……it is the VIX of crypto. The VIX of crypto right now just got off the ground in the DeFi space. It controls 60% of DeFi swaps in this space as of today.
Professional traders use volatility data to make informed decisions and be on the right side of trade. Therefore, the CBOE Volatility Index, known as the VIX, is popular with equity traders.
Bitcoin is known for its high volatility and Universal Market Access (UMA) plans to offer traders an opportunity to trade volatility in a decentralized way. I think this coin has huge potential. For that, the protocol plans to launch a uVol-BTC product that will be settled at the end of the month. Traders could use the token to speculate on the increase or decrease in volatility, or hedge their Bitcoin positions they do not want to sell during sharp corrections. Today on Feb 5, 2021 options expired on BTC and the price is moving. I expect the derivative market for BTC to skyrocket over the next ten years. If the product turns out to be successful, a uVOL-ETH token is also planned in the future.
Other than the regular synthetic tokens that track the price of an asset, traders keep looking for new opportunities that do not give institutions a direct edge. In order to cater to this demand, UMA plans to launch a new synthetic token called ‘uSTONKS’ that will be based on the ten most commented stocks on the r/wallstreetbets Reddit forum. This is another reason I am bullish on UMA. The new uSTONKS token offers retail traders a unique way to benefit from the movement of the most popularly discussed stocks on the forum.
Early discussions are also in progress to create a “Big Mac Synth” based on the index invented by The Economist back in 1986. Launching innovative tokens attracts new traders. New traders = Metcalfe effect for the entire DeFI space. Another reason that could have added to the short-term demand for UMA was the negative 15.5% annualized yield for depositing Ether as collateral to borrow USDC.
UMA has soared from an intraday low at $11.234 on Feb.2 to an intraday high at $43.998 today, a 291% gain within three days. I began buying it in December 2020.
The first batch of tokens to be listed is uSTONKS-MAR21 with 10 stocks: GEM, AMC, NOK, BB, SLV, TSLA, PLTR, SNDL, AAPL, and SPCE. UMA is launching the index in collaboration with YamFinance which is one of the most popular farming DeFi projects.
UMA price could surge even higher according to various metrics
It’s important to note that despite the recent price surge, the number of whales holding between 100,000 and 1,000,000 coins has increased by seven since January 28. Similarly, other large holders with 10,000 to 100,000 coins have also joined the network in the past week which indicates investors believe the digital asset has the potential to rise higher.
WHAT ELSE?
Aave is a digital finance app on ETH 2.0 that is building a digital trust score which is analogous to an Equifax credit score in the finance world. Aave is a money market that is attempting to establish the time value of digital assets by paying interest on the movement of things with value on Blockchains. It does not have to be just money or coins. It can also be a property that is tokenized. It is the world’s first true digital lending market in my opinion.
For example in Sept 2020, UniSwap exceeded the crypto exchange CoinBase in terms of exchange of value as a Decentralized market. That got my attention last year and I decided to look at all the players that were just beginning on the ETHER chain. How Uniswap made money was more shocking to me.
On Coinbase exchange the exchange owner gets the transaction fees from trading volumes. They also had the risk of building and funding the exchange. What Uniswap was, as if you owned their token you would share in the transaction fees directly with coin ownership because the Dapp called Uniswap would cut out the middle which in this case was Coinbase. Once I understood this I began building a position for all these companies collecting fees in swaps. Uni, UMA, AAve, Market, YFI are right now my favorite ways to play this DeFi trend. Owning them is a bet on future commerce in the DeFI space. I will say not all of them will succeed long term. Some will go to ZERO. Be aware of this. Another way I think about this speculative play is that one of these companies might become the Amazon or Goldman Sachs of the DeFi space. That excites me and I think this space might offer more upside than BTC will. But it filled with execution risks.
The person who holds the coins is getting paid as transactions go up by the value of the coin going up. In reality, it is like being paid a dividend yield. It is a new way to own a bank without the equity risk. This group of coins is actually building the Yield curve for the DeFI world. In the centralized world, these companies are worth a fortune. Right now you can buy these coins very cheaply.
The problem is knowing which one is winning the battle of supremacy. I follow the money flows to make a decision and I add to those positions. I am fully aware that 90% of these names might go to zero but I have faith that one will become the 300-pound gorilla of the DeFi space.
The biggest development I think is each one of the companies makes money every time someone buys BTC and decided to get a yield on it. Many people. like, me, are doing this. If you view BTC as pristine collateral that is growing 200% why in the hell wouldn’t the market want another 6-10% of BTC yield as the BTC sits in a cold storage vault run by YFI, as you wait for BTC to go to 1 million a coin? The way I think about it, if I want this so will a lot of others. Therefore, I want to own some of these coins.
This is a market that has no need for venture capital when you really understand it. The market is self-funding. That means this space is going to eliminate the VC in the analog market. How much is that worth?
In 2019, North America had the highest valueof VC deal funding globally, with approximately 113 billion U.S. dollars in financing. Right now these companies market cap on crypto exchanges is only 15 billion dollars. That tells me they are worth a ton more.
Can this space be used to create easy free profit via arbitrage? What is arbitrage?
Have you noticed BTC or ETH have different priceson different exchanges at the same time when you’re buying? This is how you arbitrage the price.
Arbitrage is already profitable in DeFi.
Arbitrage traders are an essential component of the Uniswap ecosystem. These are traders that specialize in finding price discrepancies across multiple exchanges and use them to secure a profit. For example, if bitcoin was trading on Kraken for $35,500 and Binance at $35,450, you could buy bitcoin on Binance and sell it on Kraken to secure an easy profit. If done with large volumes it’s possible to bank a considerable profit with relatively low risk. Uniswap and Aave do this now.
How does this actually work?
Getting started with Uniswap is relatively straightforward, however, you will need to make sure you already have an ERC-20 supported wallet setup such as MetaMask, WalletConnect, Coinbase wallet, Portis, or Fortmatic.
Once you have one of those wallets, you need to add ether to it in order to trade on Uniswap and pay for gas – this is what Ethereum transaction fees are called. Gas payments vary in price depending on how many people are using the network. Most ERC-20 compatible wallet services give you three choices when making a payment over the Ethereum blockchain: slow, medium, or fast.
Slow is the cheapest option, fast is the most expensive and medium is somewhere in between. This determines how quickly your transaction is processed by Ethereum network miners. Right now the gas fees on ETH 2.0 are high. That is great for ETHER owners because it uses ETH supply up to lower the supply and this makes ETHER less centralized the more it is used by DeFi application. So in essence I am saying these decentralized apps and tokens are what is driving ETHER real value right now. It is not ETHER itself. It is a giant feedback loop being built in the DeFi space. The more Aave, UNI, UMA, and MAKER money they move, the better it is for ETHER price.
If my thesis is correct over the next 4 years we should see ETHER price moves move away from BTC moves and it should happen after these DeFi apps keep driving capital across the DeFi ecosystem.
Now that I understand this space well I think each one of these DeFi apps is fully composable onto many other businesses that will get built on ETH 2.0. I personally think banks are going to favor ETH 2.0 because they believe it is a centralized platform they can control. DeFi apps are going to make ETH 2.0 more decentralized. So I see Aave, UMA, YFI, Maker, as the main competition for banks in the next few years. They have a huge advantage because the yields they are paying on crypto exchanges cannot be matched in conventional banking. Banks however, know when interest rates go negative money will flow out of their bank into something else. They will adopt blockchain and hope their clients use their payment rails into the world of crypto. I think they are nuts to think this way. DeFi is the best way to unbank and this is why I love these coins over the next 5 years. These coins compete with one another, but unlike banks, they fit together like lego blocks in the DeFi system and there is no longer a financial problem of Bank of America connecting with JP Morgan in this financial world. I think that is a really valuable that legacy banks won’t understand how to adapt too. I think Avanti bank in Wyoming is going to disrupt them in a big way. If you do not follow Caitlin Long you should. She is a Wall St. veteran who is now going fully digital with Avanti. She has deep ties to Kraken and to Senate banking committee via Senator Lummis.
My Take
Senator Cynthia Lummis has been assigned to the Senate Banking Committee.
Lummis has been vocally pro-digital assets in both her candidacy and since taking office.
Lummis said she plans on forming a Financial Innovation Caucus to educate her fellow senators on emerging financial technologies. She was key in changing Wyoming laws for the benefit of Kraken and Avanti who are both based in Wyoming. She is going to be a big player in the Senate for Bitcoin.
The Office of the Comptroller of the Currency (OCC) granted another crypto-focused firm conditional approval to operate as a national bank.
Protego will join Anchorage as a banking editor with approval from the federal government, according to a new announcement from the U.S. banking regulator.
Protego & Anchorage aim to serve institutional clients interested in digital assets. The Seattle-based firm plans on being a “vertically integrated and fully regulated bank built on blockchain.” Now, as a nationally chartered trust bank, it can hold, trade, lend and issue digital assets to clients. These will be its four primary services, according to the bank.
However, Protego is still in the organizational phase of development, according to the OCC’s announcement. It will have 18 months to meet the terms of its conditional approval. It will be able to convert to a national trust bank when it begins to operate. Currently, it’s a Washington State-chartered trust company.
I am not sure which lego block DeFi app is the most valuable yet, so I decided to spread my bets across a bunch of them.
This video lays out why the leaders of ETH 2.0 cannot be trusted.
Tolerance of ambiguity is a necessary condition for creativity for wealth and health creation.
Perfect money has never existed, of course until now, gold is the closest thing to it. The shiny metal might be a pet rock or a barbarous relic to some, but it has remained the most stable asset over the last 5000 years, granting stability every time monetary collapse ensues; the best candidate to replace whatever the elites claim is backing the fiat monetary system is now underway. Bitcoin is a solution outside of the governments power. I believe it will be a large part of the solution of the coming financial tsunami in the next 5-9 years in this Fourth Turning.
In the early 1800s, during the first of George Friedman’s U.S. socioeconomic cycles, the greed of the Second Bank of the United States’ stockholders created an economic depression. To enrich themselves, they issued paper currency with no backing, prompting rampant speculation, ultimately leading to a crash. (Pic of Jackson from New Orleans)
The 1837 Panic ensued as President Andrew Jackson, a sound money advocate, had responded to the speculation by backing the U.S dollar with gold and silver to purge economic deformities from the previous cycle. The economy remained somewhat stable until America fought a civil war thirty years later. Abraham Lincoln’s government committed the same economic suicide as the shareholders of the now-defunct Second Bank of the United States. That bank issued vast sums of paper currency to finance the Civil War by printing money— plus speculation on railways — drove America into yet another depression, which led to the Coinage Act of 1873 where President Ulysses S. Grant enacted the de facto gold standard to suppress malinvestment and inflation. This is where the gold standard began to end the hyperinflation of money printing.
This period in U.S. history is what American’s should expect when the next crisis unfolds today in front of eyes, only this time with a modern twist: Cryptocurrencies will be used in some way to replace gold. The next major collapse will coincide with both the mass adoption of crypto and the resurgence of commodity money in some fashion.
As paper fiat money rapidly devalues something else the elites will use will reflate the value of money. This will lead the resurgence of commodity money around the world. I expect it to be fully digital. The COVID pandemic has already begun to warn people to stop using fiat and used debit cards and credit cards and I view this as step one of the government warning the public something new is coming. They will use the pandemic to ease into a new monetary reality. I believe this is why the pandemic really was orchestrated as it has been. It provided a cover for the Treasury for us to avoid another civil or revolutionary war. I believe this is why the elites in Washington DC have made the January 6th reactions of the people so noteworthy in their response. Furthermore, I believe that is why permanent fences are being installed in the Capitol. If they did this without the events of January 6th they’d have no plausible answer why they did this.
Detractors like me, are cautioning you against the symbolism of permanent fencing surrounding the building. A government run by criminals needs protection from the “We The People”. This is precisely what Snowden and Assange have warned us about. Now we can see why lawmakers have asked for this. Lawmakers say keeping a barrier around “The People’s House” cuts against a message of transparency and accountability to their constituents. This is a farce for the Great Reset s, real agenda, monetary debasement.
Permanent fencing sends the wrong message to the nation and the world, by transforming our democracy from one that is accessible and of the people to one that is exclusive and fearful of its citizens because Congress is a cabal.
Crypto suits an increasingly technological world in which we desire speed, security, and privacy. It is programmable money and a form of digital gold. Using precious metals as a currency — trading in grams, and transporting freight loads between parties like in the California Gold Rush of 1848 — is a crazy proposal for a modern medium of exchange. Transacting with a crypto wallet beats transacting with a gold debit card, hands down.
Crypto, however, isn’t perfect money either. At best, it’s a currency without commodity backing. It is backed by scarcity and the promise of elimination of a central banks controlling arm. It removes politicians and banks control. Though we live in a society where the elites have replaced gold with debt, this doesn’t mean we must continue their mission to destroy money’s intrinsic value. We have the choice to opt out and unbank ourselves before their plan takes effect. As history shows, we need a gold-backed currency to reverse the sickness that fiat currencies have inflicted on society, and to have any chance of preventing elites from siphoning off wealth for themselves via monetary manipulation.
Only when the great reset occurs — where the fiat system relinquishes, and money regains its value, meaning, and purpose — will we know whether this new monetary paradigm will be governed by the people for the people, or by the same type of elites who always finds a way to exploit the system. It’s obvious which outcome will create a better, fairer, juster world, but it’s also clear, based on history, that the power will end up in the hands of a more autocratic, digitally empowered elite. Is this the moment when the people finally rise up and take charge? We’re about to find out. Is BTC packing your parachute, because it is packing mine. I have lost all faith in the Fed and US Treasury.
I believe the day Decentralized medicine was born was the day the Nobel Prize in medicine was awarded in 2017.
What is cool about bringing old science to new eyes by putting windex on the glass eyes of medicine?
Your certificates, degrees, status and wallet do not matter. How you treat your equals and people under neath your direction matter most. Doctors and patients are not speaking the same language to one another because they both suffer from the same ecologic deficits these days, while have a different educational paradigm of beliefs = They are both chronically disconnected from circadian biology and nature. Doctors were schooled in a centralized system which is their algorithm of understanding. Their customers are not biased in this way. They get this information for free, and this makes them the product being sold to the industrial healthcare complex.
If I can get one in hundred physicians and patients to see this perspective, then I am doing OK. This new project I am involved with on Quantum Health TV aims to inflate these ideas for physicians to build a new decentralized medical system.
Medical school 25 years ago could be considered an algorithm controled by a curriculum. This curriculum allowed maximum human intervention. It did not allow machines to take data and then decide for patients.
Algorithms: For those in non-procedural medical fields it’s our thought process we offer our patients. And rigorous logical medical thought is becoming scarce, I fear because they are importing our knowledge base into algorithms and the output of algorithms continues to morph because machines continue their algorithm variance. There is no control. We are now training medicine residents that will easily be replaced by midlevel practitioners who haven’t gone to medical school but know how to apply algorithms in recipe format.
But everyone forgets the outcome of algorithms continue to evolve long past the day they were created.
What we fail to realize is that contemporary technology permits decentralization, it also permits centralization via algorithms when they go unchecked by human critical thinking. It depends on how you use the algorithmic machine learning and how you let machine learning use you.
Decentralized medicine is mitochondrial based and involves significant physician input. The key issue for medical students and young physicians, is can they hope to capture a job in DeMed platform in the future? Can they do this without going through 10 years of debt creation and a centralized educational format taught in training? I have found they can if the are connected to the digital monetary network to power their careers as early as possible. This creates freedom to untether from the centralized hospital system.
Can you imagine living in a world where executing a care plan or operation, buying an original idea to solve cancer, or accepting payment from a patient can be done without needing trust? We might be in position to just trust the code of a blockchain? No third party, like a hospital or insurance company is required?
What is obvious is hard for those with a bias to accept. There are two kinds of people in this world. Those who think the government is doing things in their best interests and those who think critically, to make our world a better place.
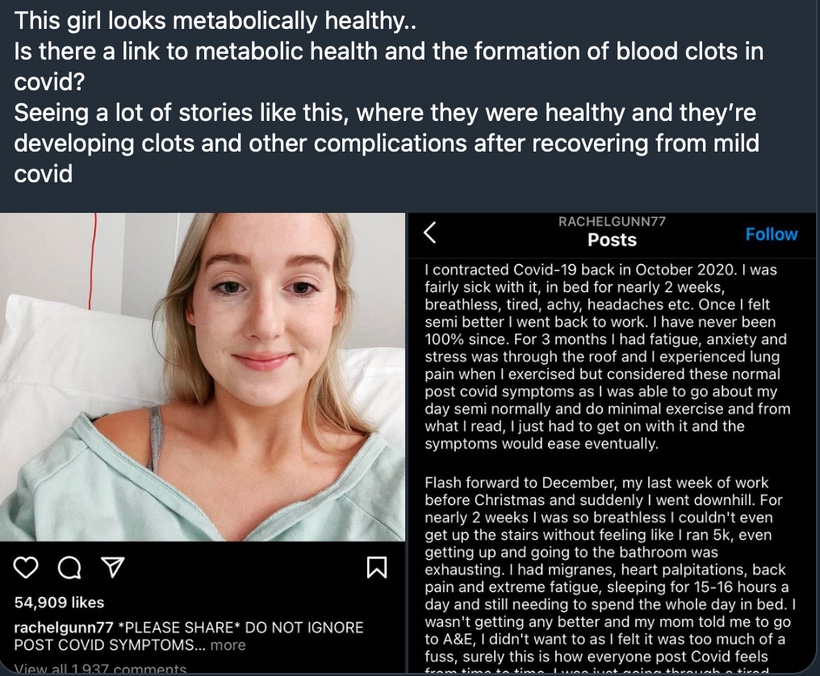
Pictures like this below make sense to a decentralized doc, but not to a centralized one. Are you really healthy if your blood clots when you get a virus? Centralize docs have no idea how the lack of a proper Coulomb force can lead to clotting in COVID. Coulomb force, also called electrostatic force or Coulomb interaction, is the attraction or repulsion of particles or objects because of their electric charge. When people clot platelets charge has changed for some reason found in our light environment. Electric charges cause electromagnetic force fields around them. This causes things to do the things they do.
Coulomb forces must be balanced after daytime and this occurs at night when light is absent. This is why light at night is so bad for us, and why a centralize doc has no ability to figure out why this girl clots her blood after becoming exposed to a weak virus. Does this tell you something deeper about humanity now? Why are humans dying from a weak virus now? A decentralized doc gets it…………do you?
We see the world as what we carry in our own hearts. When others see mistakes, I observe a lesson.
They see a shadow, I observe the light that casts it.
They see the night, I observe the moon and its effect from the Earth’s tilt and how it varies the Coulomb force. They see a corporation, I observe people who make it thrive and die. They see millennials as a problem, I observe our bright future. They see success, I observe the coming journey. They see me as a stranger. I observe them, as my future friend and cohort in mito-hacking for a better world.
^^^^^^^WHY IS THIS AN ACCURATE DECENTRALIZED VIEW POINT?
Melatonin is created by the Coulomb forces in AM sunlight. Melatonin levels vary within tissues because of how much light tissues get. As a result, it appears melatonin is a guardian of the Mitochondrial genome (37 genes). Out of the 37 gene, 13 of them are specific to energy-transforming mitochondrial genes. Those 13 genes only code for the proteins that tunnel electrons and spit protons out of the mouth of cytochrome proteins. The mitochondrial genome undergoes 3 times as many genomic mutations as the nuclear genome by design. Melatonin levels are critical in monitoring mitochondrial behavior and light energy transformation by controlling how energy is being transformed from light to create physiologic power.
The major function that melatonin helps smooth-out in mitochondria are
Energy metabolism and flux via control of electron and proton tunneling.
Redox balance within the mitochondria = GSSH
Ion homeostasis = electrostatic controls via Coulomb forces that vary via light
The signaling of cell death and mitophagy = % heteroplasmy in a mitochondrion = the amount of light energy transformed to physiologic power.
This picture defines the centralized system. In the decentralized system There are over ten metrics to evaluate thyroid function. Centralized testing looks at two. If those two are within normal limits, “you don’t have a problem”. You get handed a Rx for an antidepressant and synthroid.
The only way to fix the the medical system is to build a decentralized one where no one on the treatment side of care has ultimate control but the patient. The relationship between doctor patient must be repaired. Three mechanisms in which decentralization impacts on health system equity, efficiency and resilience are:
1. ‘Voting with feet’ reflects how decentralization either exacerbates or assuages the existing patterns of inequities in the distribution of people, resources and outcomes in a jurisdiction.
2. ‘Close to ground’reflects how bringing governance closer to the people allows for use of local initiative, information, feedback, input and control.
3. ‘Watching the watchers’ reflects mutual accountability and support relations between multiple centers of governance which are multiplied by decentralization, involving governments at different levels and also community health committees and health boards
Where others see nothing or impossible strings………I observe decentralized answers. We have to cut the umbilical cord physicians have with centralized systems to get to the level of understanding how environmental light controls reality we observe. That won’t be easy because most physicians are now paid by that system. Physicians must plug into the BTC monetary network before they cut their umbilical cord. The more physicians become employed by fiat payors the more subject patients will be to corporate medical algorithms. These computer generated prescriptions will determine your health outcome. You and your doctor lose their power to help reverse the disease.
The current centralized payment structure reinforces the focus on disease by rewarding procedures, not cheaper interventions like prevention or care coordination. They never pay for therapies that hold the promise of disease reversals.
In the 1950s, 60s and into the 70s, primary care physicians were well respected members of the community and helped patients navigate and coordinate more specialized care. Children of this era remember having a family doctor who would attend to all of their family’s medical needs.
In the 1980s and 1990s when I was in medical school I was affected by how the system incentivized care, as the cost of healthcare became burdensome for corporate and government payers, the dynamic changed. The federal government and the insurance companies created a structure of procedures and payment rates for each. Procedures based on higher levels of training and technology received higher fees. The Feds and insurers tried to push down prices of procedures, but at the same time they rewarded advances in medical knowledge and technology, and the result was highly trained specialists were well paid for performing sophisticated procedures, and family doctors were squeezed. This trend was a driver in my own decision tree back then on what career path I should choose.
IMPLICATIONS
As a result of the centralized system, treatment decisions are influenced by money, not necessarily what is best for the patient. The procedure-based payment structure rewards doctors for doing more, even when it might be better to do nothing. I know this first hand. This is still true in 2021 for complex spinal surgery.
Our healthcare delivery system spends more than 700 billion of its 2.3 trillion in annual health spending on medical care that does nothing to improve a patient’s health…seven hundred billion dollars every year. And, most alarmingly all that ineffective treatment and harmful care represents one-third of tests, treatments and procedures that physicians perform.
Our current centralized reimbursement system and our cultural values serve up a ready answer to physician uncertainty as to what tests and treatments to order for their patients: more is better. When evidence is incomplete or conflicting about when to use a particular procedure, surgery or diagnostic test…some physicians will treat more aggressively, especially if piecework reimbursement rewards that.
The implication: Unfortunately, only about 20 percent of clinical procedures have solid scientific evidence to back them up. This means in many case physicians are flying blind and under great economic pressure to do more, even when it doesn’t necessarily serve the patient’s needs. With an arsenal of government-approved treatments available that are paid for in a centralized manner, there is great temptation to do “something,” even when it might be better to simply watch and wait. I saw that unfold in my own practice for 25 years.
With money flowing to specialists, primary care doctors were forced to see more and more patients and had less time to spend with any one patient. Unpaid services such as preventive care and care coordination quickly went out the window. With the lure of greater prestige and earning potential, medical students funnelled into specialties, creating a deficit of primary care doctors. Today, it isn’t unusual for patients to be shuttled from one specialist to another with no one looking at the bigger picture of the patient’s well-being. This process has gotten larger over my career. Patient outcomes have gotten worse.
Most of you know my specialty is neurosurgery, and within it, I subspecialize in spinal reconstruction. You would think, from this position I have obtained I would support centralization. The position has allowed me to see the problems clearly. This position showed me that centralized power in medicine is an impediment to health of people. This is why began to speak out against this centralized model of care 15 years ago. My personal perspective is the generalist in science always is the most valuable specialist. They know more so they connect more dots to lead to a new understanding to get health back.
In centralized medicine patients’ preferences, goals and values are marginalized.
When the patient is reduced to a vehicle for disease, the doctor becomes the most important person in the healthcare process. This may work fine when medical decisions are straightforward. In acute diseases they are. In chronic disease management they are not.
When there is ambiguity, a patient’s preferences, goals and values are essential in choosing the right course of action. This is a strength in a decentralized paradigm. The current centralized culture of medicine, in addition to the economic incentives mentioned above, doesn’t encourage this kind of two-way communication.
The discussion about norms and values inherent in every clinical judgment and decision seem to shift from the doctor’s consultation room to the conference room of the doctor’s professional association. If intentionally or unconsciously physicians do not want to negotiate with their patient about the usefulness of certain interventions, they can refer to the opinion of their professional association that is codified in guidelines and protocols instead, thereby shifting the responsibility for clinical decisions from a personal decision to a professional group decision. That is a deep centralization problem.
All too often, the patient buys into the mindset that decisions about their health are best left to evidence based paradigms of associations. Patients become passive recipients, rather than active participants in their own care. This may have been acceptable when the aim of medicine was simply to keep people alive, but chronic conditions, in particular, require the patient to play a larger role in managing their own health.
Adding fuel to the fire is a rising tide of chronic illness. Simultaneously, the Baby Boom generation, which represents a quarter of the U.S. population, is beginning to hit retirement age. This is a period of life when we become more vulnerable to illness and chronic conditions tend to accumulate.
As we’ve seen, the disease-based and doctor-centered medicine that brought us so far in the 20th century isn’t well equipped to mitigate and manage this growing tide of chronic disease. A new decentralized paradigm is needed that treats the whole patient and establishes a more balanced relationship between doctors and their patients.
Today, in medicine progress is measured by the speed at which algorithms can destroy the conditions that sustain life. Those narratives are pushed on social media as evidence based by doctors and researchers employed by the centralized system. The evidence of the fidelity of those “evidence based ideas” are found in the abysmal results of our chronic disease epidemics that the centralized system.
Our centralized healthcare system in the 21st century focuses on treating diseases, not people. The medical knowledge we gained in the 20th century had very narrow goals: stop people from dying. It was focused on treating short bouts of illness caused by a specific disease often localized to a particular organ or organ system. However, the CDC estimates that over half of adults in the U.S. suffer from one or more chronic diseasesthat cannot be cured, only managed via machine learning algorithms. The costs of treating these diseases now represents 75 percent of the $2.3 trillion in U.S. annual healthcare spending.
The centralized system fosters these beliefs………..Do you?
I know I do not.
DECENTRALIZED MEDICINE IS A SOLUTION
We can use algorithms as an aid to the systems of our society, like pilots use autopilot or how we use cruise control in our cars, but we must never let them run our society completely on their own – the day we do, will be the day we fall.
The right thing isn’t always real obvious to the rest of the world. Sometimes the right thing for one person is the wrong thing for someone else. And everything, in retrospect, is obvious to those who use forethought. How you think makes you great. 99.9% of humans use hindsight to dictate their actions. Hindset in medicine is dangerous. We have let the industrial healthcare complex take over decision making and no one is questioning the problems with it. Some of us train to observe the unseen first. We learn to ignore what the eye sees and focus on what the brain observes. This is how the decentralized mind sees problem solving.
Like most things in life, everything is great— until it isn’t. Circadian destruction comes from bluelight and nnEMF and this has created our chronic disease epidemic reality.
DeMed is the ‘counterintuitive” antidote for nnEMF ecocide caused by technocracy. With ecocide being the irreversible destruction of our natural environment by electropollution.
The irony of modern society is that we are now the best-informed society that has ever walked this planet, but yet we also carry the greatest risk of dying from our own ignorance. Technology allows for escapism from nature. Being divorced from Nature is where all diseases begin. But technology can be harnessed to change medicine just as easily.
This is why good people can make tragic errors for people who follow them. Think employed docs and patients.
Case in point below.
How does a half-truth about food lead to a full lie in reality? The LCHF folks say this: Increase fructose load increases uric acid which inhibits the production of nitric oxide constricting blood vessels to the brain. Is this true?
Recent literature shows that uric acid is actually protective to damaged human brain tissue. So how come the LCHF physicans got it all wrong?
Did they see the whole truth or just the truth they understood from their centralized education?
The reality of the entire picture: Fructose shows up in foods grown by nature that only grow in strong photosynthetic environments naturally which have full-spectrum sunlight. So fructose is never designed to be present without strong solar UV/IR exposure. Nitric oxide is also made by short wavelength UV light, so who cares if fructose inhibits Nitric oxide? Nature always couples them…………..
The only people who do care are people eating an LCHF diet who live indoors way too much. They never get nitric oxide from their skin because they are rarely in it to experience it so their physiology is tuned the way nature designed. This is also why they get fat. The subcutaneous fat in humans responds metabolically and hormonally to sunlight or the lack thereof. Sunlight affects the Coulomb charge of our bodies. It just so happens sunlight increases Nitric oxide production to offset the loss in foods with fructose. So it is really a lack of sunlight and not the foodstuff that is the real problem. These physicians never get to this level of understanding because of their centralized education that was paid for by Big Pharma and the Industrial healthcare complex.
Big Pharma is not interested in cures, just creating new customers. This is why blue check MDs are dangerous for the public. They never ask the right questions for you because of the algorithms that were uploaded to their minds in training. Critical thinking has atrophied in physicians who have been trained using corporate algorithms.
Medicine is now a tech industry where clinical nuance is dead and the centralized algorithms of the health lobbist rules public health.
Decentralized medicine allows the doctor to examine the algorithm and critique with by holding the coding outcome up to Natures rules to limit the risk of disease.
Why do I love writting my ideas down for you? I enjoy self-publishing & sending researchers and clinicians copies of my blogs. What these blogs represent are rejection letters for the paradigms beliefs. When these clinicians and reearchers read my work, they respond, ‘Who is this guy?’
And I’m like, ‘the end of your industry.”
Decentralized medicine is a virus worth spreading.
SUMMARY
Blockchains allow humans to connect weird things together
Many people even today do not understand how we can create a software of silicon to hold a greater value than gold. That is BTC in a nutshell.
How can blockchain technology bring value to medicine?
Communications is at the heart of medical e-commerce and community. Telemedicine has exploded on the scene because of COVID. Soon physicians will be paid in Satoshi minute by minute for their value. Apps like Strike will facilitate this transition. Banks like Avanti will fuel our practices. They are building on and off ramps we will need to build the practices our patients need.
The global eCommerce market poised to reach $135 billion by 2023. The introduction of blockchain technology in eCommerce helps build a global decentralized economy. Medicine has to be part of this. It is projected that within a decade crypto could be a mainstream alternative to cash and cards.
Physicians need to know the consumer’s appetite for crypto payments is influenced by good publicity, ease of use and convenience. They’ll never get this experience as an employee in a hospital. For merchants and retailers, crypto payments will likely be an add-on to existing systems. One thing we can agree on is the payments industry is dated and ripe for disruption in medicine. Physicians should embrace this chaos and not run from it.
Physicians have to become capable of accepting and processing cryptocurrencies. It will foster “a marriage between inventory management and exchange platform.” This decreases physicians needs for centralized systems of support. Blockchain technology is capable of handling virtually the entire eCommerce experience for physicians who go out on their own. This includes product searches, supply chain tracking, loyalty programs, product reviews, data security, and post-sale customer care.
Blockchain technology facilitates verification and trust while eliminating the need for a middleman. In the case of medicine, the application reduces the dependence on Big Pharma and researchers who perform useless science and useless papers, and electronic medical records. The blockchain ledger will help us keep an accurate database of a work’s provenance on the blockchain. This data can be monetized by patients and physicians and not by Google or your hospital.
DeMed physicians will be the innovators of this paradigm shift. The forward thinkers and risk-takers are necessary in every technological advancement and revolution. Many of these ideas will fail and billions of dollars will be lost and dreams shattered. From these attempts, the best of the best will rise, and change how we live, work, learn and play. Failure is always the first step to success. I know. I have been failing at this paradigm shift for 15 years but I refuse to give up on this idea. Success in building this new practice is stumbling from failure to failure with no loss of enthusiasm
I believe the world is ready now for this idea.
The current GME stock squeeze situation and DeMed are linked. Do you see the link yet?
The moral of the story of GME is that retail Reddit investors, for better or for worse, finally learned how to weaponize options and the short squeeze operation using leverage. lt is likely going to lead to the utter destruction of the current centralized markets beginning today, thus, setting the stage for globalized decentralized markets that are fueled by BTC monetary network.
Doctors and nurses need to find how to optimize the BTC monetary network to power their successes while limiting their own destruction at the hands of corporate algorithms, medical schools, residencies, and hospitals. So when your monetary network is inflated, no person or employer can force you to vaccinate yourself or do something to a patient that breaks Nature’s laws for mitochondrial function.
DeMed defends chaos. Decentralized systems are the quintessential patrons of simplicity. They allow complexity to rise to a level at which it is sustainable, and no higher.
American federalism was the embodiment of political tolerance and decentralization – the expression of the liberal conviction that society can manage itself and needs no central plan.
American medicine before the AMA was the embodiment of political tolerance of ideology with no central recipes. Where patients can manage their diseases when reintroduced into Nature.
The purpose of a centralized medical system or any other system, is not to ensure stability in people, but to exploit people in the society. It is time to change the paradigm.
Physicians and nurse interested in transition planning can join me for brainstorming sessions on how to get the logistics right at kruseatdestin.com. DeMed amateurs talk tactics. Professional DeMed users talk logistics.