The short answer is they are not. This post is a scientific post of why they are not linked. The outcome that supply and demand are not linked to price is found in the picture above from live on-chain data. Nicholas however, did not believe the on-chain data was accurate. This is when I decided to go deeper for the answer. This post was created because of a conversation that occurred on ClubHouse between a gentleman name Nicholas and myself in Crypto N Coffee.
Wisdom is knowledge applied.
The internet of wisdom is found by challenging everything you believe right now using nature’s laws.
Wisdom is knowing what not to think about any longer……..
Are humans wise? We have named ourselves Homo sapiens—‘wise person’. It is clear that as a species we have taken control over the environmental and biological future of Earth. Maybe Homo dominatus—which translates as ‘dominant person’ or ‘tyrannical ape’—would be more apt???
Wisdom and knowledge are not synonyms. Knowledge/data is fundamentally useless until it is connected by nature’s blueprint to become crystallized into a coherent organization.
Whatever matter actually does itself, ironically doesn’t matter. Matter needs light to tell it what to do. It is the information linking matter which is primordial. Water = alphabet magnetism = circuit board, light is the photo-electric current that carries the information and energy matter requires.
Wisdom and knowledge are not synonyms. Those who seek wisdom must seek many truths to gain insight. They must be tenacious. Knowledge is a part of ignorance that man arranges and classify. Knowledge has the shelf life, like fish do in a market.
Common sense is that supply and demand have to be linked to price. Is this true based on what we know today?
It is not.
It is not sustainable and does not always lead to truth. If knowledge is information, wisdom is the understanding and application of that knowledge and insight is the awareness of the underlying essence of a truth.
Sadly we can gain a lifetime of knowledge, yet never see the wisdom in it. We can be wise but still miss the deeper meaning of facts. Today, Bitcoin price is a good example of this.
BITCOIN IS A DIGITAL INFORMATION NETWORK = VOPSON PARADOX
Because it is, this explains why its supply and demand are not linked to price. Sounds very counterintuitive doesn’t it?
WHO IS VOPSON? WHAT IS HIS PARADOX ABOUT? HOW DOES IT SCALE TO BTC?
Dr. Melvin Vopson of the University of Portsmouth, in the UK, has a hypothesis he calls the mass-energy-information equivalence. It states that information is the fundamental building block of the universe, and it has mass. This accounts for the missing mass within galaxies, thus eliminating the hypothesis of dark matter entirely. Not only does his paper explain why dark matter is a bad idea, it also explains why price is not always coupled to supply and demand.
WHERE DID VOPSON’S IDEA COME FROM?
In 1933, Swiss astronomer Fritz Zwicky, while observing the motion of galaxies in the Coma Cluster, began wondering what kept them together. There wasn’t enough mass to keep the galaxies from flying apart. Zwicky proposed that some kind of dark matter provided cohesion. But since he had no evidence, his theory was quickly dismissed by conventional science of his day.
Then, in 1968, astronomer Vera Rubin made a similar discovery. She was studying the Andromeda Galaxy at Kitt Peak Observatory in the mountains of southern Arizona when she came across something that puzzled her. Rubin was examining Andromeda’s rotation curve, or the speed at which the stars around the center rotate, and realized that the stars on the outer edges moved at the exact same rate as those at the interior, violating Newton’s laws of motion. This meant there was more matter in the galaxy than was detectable. Her punch card readouts are today considered the first evidence of the existence of dark matter in astrophysics.
HOW DOES VOPSON DARK MATTER PAPER LINK TO BITCOIN?
The bitcoin network is a peer-to-peer payment network that operates on a cryptographic protocol. Users send and receive bitcoins, the units of currency, by broadcasting digitally signed messages to the network using bitcoin cryptocurrency wallet software. Transactions are recorded into a distributed, replicated public database known as the blockchain, with consensus achieved by a proof-of-work system called mining. PoW systems requires energy input and when a transaction is submitted to the Bitcoin network, the information is passed on through all Bitcoin nodes—all computers connected to other computers in the blockchain—at the same time (through the blockchain).
In this way, BTC functions much like a public ledger, accounting for economic transactions and providing a way to verify that all Bitcoin users have been equipped with the same information. Everyone can download a copy of the blockchain and use it to trace the path of Bitcoins from one Bitcoin transaction to another. (It should be noted that although there is a record of every Bitcoin transaction ever made, they are linked to a specific Bitcoin address, rather than a personally-identifying name or email. For this reason, Bitcoin is considered pseudonymous.
Proof of Work blockchains codifies that an information transfer has happened. In 1961, Landauer first identified the link between thermodynamics and information theory by postulating that the logical irreversibility of a computational process implies physical irreversibility. His idea indicates that information is a physical quantity in digital systems, his idea demonstrated the link between information theory and thermodynamics.
The goal of a blockchain is to allow digital information to be recorded and distributed to every participant, but never edited.
If the blockchain is editted information is destroyed. Rolf Landauer paper predicted that erasing even one bit of information would release a tiny amount of heat. His theory has been experimentally validated many times. It is OPERATIONAL in the digital world and BTC code is part of the digitial world. What are the thermodynamic implications of Landauer’s paper for Bitcoin price?
A loss of heat = lowered hashrate = lowered price. This is why the recent Chinese miner re-deployment has affected price without having any on chain affect to supply. I tweeted this pic below out to the creator of the Crypto N coffee room. I decided to make this blog post after researching the topic of how information loss could affect price without affecting demand. Landauer’s paper proves why Nicholas conventional advice is not operational for Bitcoin.
When heat is lost as energy, mass must also be lost from the network according to Vopson recent paper extending Landauer’s idea from 1961. As mass is lost, the lever of BTC effect on other financial instruments would decrease. The loss of mass shows up in Bitcoin by a loss in price. This likely would affect the price until information loss from the hash rate change stabilized. The hash rate is equivalent to the metabolic rate of the digital algorithm that is BTC. In this way, it mimics what a lowered T3 hormone level does in human thyroid.
BITCOIN IS NOT ABOUT GAME THEORY: IT IS ABOUT WHERE INFORMATION THEORY AND THERMODYNAMICS INTERMINGLE.
PoW is fundamentally more decentralized and censorship-resistant than PoS because of how it handles information. With PoW, cheap energy is the strongest determining factor in participating in transaction selection. With PoS, wealth is the determining factor. Cheap energy is far more distributed than wealth but energy networks must always preserve information to keep this relationship intact. When the hashrate drops, information is lost in PoW Bitcoin blockchain. This decouples price from supply and demand.
Decentralization links chaos and order ONLY when information is conserved.
Nature is a 100% decentralized energy network. The burden of performance NEVER ENDS within this organizing principle.
Is BTC like Nature?
Only when information on its blockchain is conserved by the network by a healthy hash rate. This implies within Bitcoin supply and demand are not linked.
As an analogy, If Proof of Work blockchains are Troy, Hashrate is its Trojan Horse.
Game theory vs information theory.
Both disciplines have a far-reaching impact on modern science and society: Information theory underpins the creation and the engineering of the digital age; game theory informs economics and social sciences. Bitcoiners believe that BTC is all about game theory. It is not.
Why?
INFORMATION:
To be clear, the idea that information is an essential building block of the universe isn’t new. Classical Information Theory was first posited by Claude Shannon, the “father of the digital age” in the mid-20th century. The mathematician and engineer, well-known in scientific circles—but not so much outside of them, had a stroke of genius back in 1940. He realized that Boolean algebra coincided perfectly with telephone switching circuits. Soon, he proved that mathematics could be employed to design electrical systems.
Shannon wrote about the code algorithm concept in a 1948 paper entitled “A Mathematical Theory of Communication.” For the first time ever, he explored the idea of quantifying the previously qualitative concept of communication, transforming it from nebulous to numerical. He used the thermodynamics of light as his backbone idea in the paper. Shannon did this by connecting the well-established measures of probability (statistics = quantum probabilities) and entropy (thermodynamics = transformation of energy) to a new measure of communication, called information. Once Shannon connected these dots mathematically, it opened the door to signal processing, compression, and converting messages into an algorithm code to transmit them digitally.
Shannon was hired at Bell Labs to figure out how to transfer information over a system of wires. He wrote the bible on using mathematics to set up communication systems, thereby laying the foundation for the digital age. Shannon was also the first to define one unit of information as a “bit.”
There was perhaps no greater proponent of information theory than another unsung paragon of science, physicist John Wheeler. Wheeler was part of the Manhattan Project, worked out the “S-Matrix” with Niels Bohr and helped Einstein develop a unified theory of physics. In his later years, he proclaimed, “Everything is information.” Then he went about exploring connections between quantum mechanics and information theory.
He also coined the phrase “it from bit” or that every particle in the universe emanates from the information locked inside it. At the Santa Fe Institute in 1989, Wheeler announced that everything, from particles to forces to the fabric of spacetime itself “… derives its function, its meaning, its very existence entirely … from the apparatus-elicited answers to yes-or-no questions, binary choices, bits.”
Wheeler’s ideas have been expanded recently by Vopson who says:
If there is no dark matter in the universe than information must carry mass in the world.
Vopson, mentioned above, took Wheeler’s notion one step further and it explains why demand and supply are divorced from price in the Bitcoin ecosystem.
His paper says that not only is information the essential unit of the universe but also that it is energy and it has to have mass. To support this claim, he unifies and coordinates special relativity with the Landauer Principle. That principle is named after Rolf Landauer who I mentioned above. Because, Landauer predicted that erasing even one bit of information would release a tiny amount of heat, a figure which he calculated. Landauer said this proves information is more than just a mathematical quantity. This connects information directly to energy. PoW is an energy consuming blockchain. Through experimental testing over the years, the Landauer Principle has held up. Now we can see this effect in Bitcoin’s price action as Chinese miners have been banned.
Landauer first identified the link between thermodynamics and information by postulating that logical irreversibility of a computational process implies physical irreversibility. This indicates that information is truly physical and demonstrates a hard scientific link between information theory and thermodynamics.
Remember BTC code is all about being a ledger of information. This means VOPSON’s new ideas link to Bitcoin.
If information is energy, Information, once created has to “finite and quantifiable mass.” to satisfy the mass equivalence equation of Einstein (E=mc^2) It so far applies only to digital systems, but could very well apply to analogue and biological ones too, and even quantum or relativistic-moving systems. Bitcoin’s ecosystem is one such digital system. I’m sorry to break it to you Nicholas, but science has definitive proof that price can be independent of supply and demand when information is lost for some reason. I’d like to thank Nicholas for tickling my curiosity to find the answer why price is not linked to supply and demand in Bitcoin. This blog scientifically explains it.
New data must be assimilated to form new ideas.
This blog shows you wisdom and knowledge are not synonyms. Those who seek wisdom must seek many truths to gain insight. They must be tenacious. Knowledge is a part of ignorance that man arranges and classify. Knowledge has the shelf life, like fish do in a market. It is not sustainable and does not always lead to truth. If knowledge is information, wisdom is the understanding and application of that knowledge and insight is the awareness of the underlying essence of a truth.
Sadly we can gain a lifetime of knowledge, yet never see the wisdom in it. We can be wise but still miss the deeper meaning of new facts on our old ideas. Today’s blog is a good example of this using Bitcoin price as an example.
There are many who know things among us on ClubHouse, but they maybe lacking in wisdom because they have not added in new data that changes what we used to believe. Your mentors should be filled with wisdom because they will be the connectors of life.
Their insight will be indefatigable for you. Not even ‘father time’ can destroy the natural truth of Mother Nature.
Creativity, which is the evocative visual storytelling of Nature’s recipes, come at a price. Consider becoming a member of my tribe at KruseatDestin.com to find out how much time you have to sacrifice for your technologic addictions. Once you do all my Patreon blogs are included in that entanglement. I want to take your health game to new levels. Are you ready?
This blog contains the mechanism to why I think the COVID vaccine is causing damage to those who get it. It is not what the anti-vaxxers think. The mechanism is 100% mitochondrial in nature. Let us get to it.
Growing evidence suggests that people with cancer and other conditions that challenge their immune systems may be incubators of mutant viruses. How?
Did you know that damage to DNA in a cellular organelle called the mitochondrion triggers an immune response in the nucleus? Mechanistic insights into this process shed light on how organelles communicate.
Mitochondria are membrane-bound organelles that act as hubs of metabolism and of innate immune signaling in cells. Each mitochondrion contains several copies of the mitochondrial genome (mtDNA), which can be damaged by extrinsic environmental stressors or intrinsic genetic mutations. This can cause degradation of the mtDNA, reducing the total number of mtDNA copies in the organelle and so leading to mitochondrial dysfunction. In addition, healthy mitochondrial function relies heavily on the crosstalk between mitochondria and the nucleus. Writing in Nature, Tigano et al. uncover a mechanism by which cells sense toxic mtDNA damage to initiate an immune response in the nucleus.
Conditions of acute stress, such as viral infection or irradiation, can lead to the activation of pro-death (apoptotic) pathways in the cell. Mitochondria have a key role in these pathways. Pore-forming proteins called BAK and BAX accumulate on the mitochondrial membrane, leading to the release of cell-death factors from the organelle into the cell’s cytosolic fluid through a process called mitochondrial herniation. In some instances, cell-death factors are not activated, in which case mitochondrial contents such as DNA and RNA are instead released into the cytosol. The accumulation of cytosolic mtDNA and mtRNA initiates a potent antiviral response. But precisely which aspects of mitochondrial dysfunction lead to the extrusion and accumulation of this mitochondrial material has been unclear.
Tigano et al. set out to examine one form of stress: cleavage of mitochondrial DNA. The group manipulated mammalian cells using ‘molecular scissors’ constructs called mitochondria-targeted TALENs (mTLNs), which generate double-strand breaks (DSBs) in mtDNA. They used RNA sequencing to analyze changes in gene expression in cells treated with mTLNs, and found an increased transcription of nuclear genes involved in the innate immune response; these included interferon-response genes, which are typically involved in combating viral infections. The authors also found that the transcription factor STAT1 was modified by phosphate groups and relocated to the nucleus — a key part of the interferon response.
Breaks in mtDNA that occur through other means, such as treatment with toxic, DNA-damaging agents or errors in replication, often lead to compromised organelle function. But Tigano and colleagues found that the mTLN treatment reduced the number of mtDNAs by only around 60%, which did not seem to have an immediate impact on mitochondrial function. The group observed no changes in key indicators of normal mitochondrial function, such as morphology, the gradient of protons (H+ ions) across the membrane, and the generation of reactive oxygen species. These data indicate that mitochondrial DNA cleavage is a key trigger of antiviral responses.
Next, Tigano et al. set out to identify the signaling molecules that relay the message of mtDNA instability to the nucleus. Although the mTLN-treated cells had intact mitochondrial function and were not apoptotic, the group showed that BAK–BAX pores did form on the membrane, consistent with mitochondrial herniation. The authors found that mtRNA — but not mtDNA — accumulated in the cytosol of these cells. The mtRNA molecules were detected by an RNA-sensing protein called RIG-I, which is better known as a sensor of viral RNA in the cytosol.
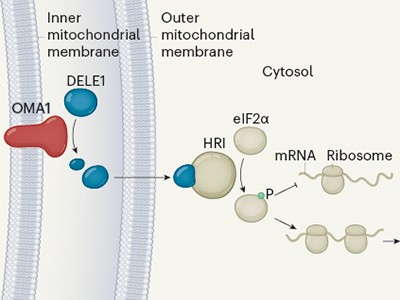
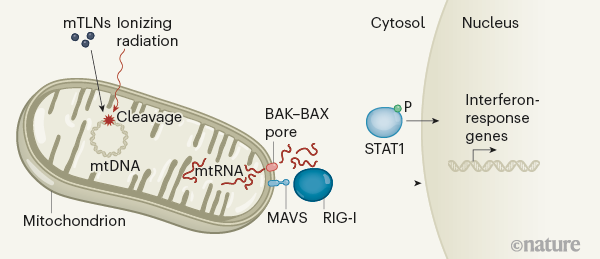
Working with its adaptor protein on the mitochondrial outer membrane, dubbed mitochondrial antiviral signaling (MAVS), RIG-I triggers a signaling pathway that activates interferon-response genes in the nucleus. These findings point to a framework by which cells engage mitochondrial signaling molecules in immune-surveillance mechanisms (Fig. 1).
Figure 1 | Communicating damage between organelles. Tigano and colleagues report a mechanism by which damage to DNA in an organelle called the mitochondrion is communicated to the nucleus. The group induced mitochondrial DNA (mtDNA) breaks, either by using ‘molecular scissors’ constructs called mitochondria-targeted TALENs (mTLNs) or through ionizing radiation. These treatments trigger the release of mtRNA into the cell’s cytosol through pores comprising BAK and BAX proteins. Two proteins — the cytosolic RNA sensor RIG-I, acting with its adaptor protein MAVS — sense the mtRNA, triggering signaling pathways that lead to the upregulation of genes involved in an immune response called the interferon response (dashed lines indicate an indirect effect). In addition, the transcription factor STAT1 is phosphorylated (P), and moves to the nucleus, where it might have a role in activating interferon-response genes.
DNA-damaging agents such as radiation, which is used to treat cancer, elicit a systemic immune response that is thought to be driven by DNA damage in the nucleus. Tigano and colleagues found that radiation depleted mtDNA numbers by 40% and elicited the same immune response as mTLNs, suggesting that DSBs occur in mtDNA as well as in nuclear DNA following irradiation. Strikingly, induction of the interferon response during irradiation was nearly completely abrogated in cells lacking mtDNA. This observation indicates that mtDNA damage caused by radiation can be a driver of interferon responses. Of note, the induction of several other innate immune responses still occurred in cells lacking mtDNA, suggesting that depletion of mtDNA specifically impairs the interferon response.
The study highlights an immunostimulatory role for mitochondrial RNA. However, questions remain. For instance, mtRNA molecules are highly unstable in nature — how are mtRNAs stabilized so that they accumulate in the cytosol, as was observed in the current study? Another avenue for further investigation is the factors that stimulate the formation of BAK–BAX pores following mtDNA breaks. It would be of broad interest to study whether drugs that inhibit this pore formation can suppress an inflammatory immune response. The discovery of a mechanism by which cells recognize self-RNAs from mitochondria to initiate an immune response also raises the question of whether this pathway might be involved in autoimmune disease. Finally, it would be exciting to explore whether artificially induced mtDNA damage could be used to increase the efficacy of targeted immunotherapies for cancer.
COULD THIS BE WHY THE COVID VACCINES ARE A PROBLEM?
Short answer……….yep.
Recall from above, mitochondria are membrane-bound organelles that act as hubs of metabolism and of innate immune signaling in cells. Tigano’s paper give us the mechanism of how mRNA engineering in the vaccines can go awry.
The current mRNA jab trials with emergency approval selected a dose that was too high, too far up on the sigmoidal dose-response curve – so we should expect a higher incidence of adverse events. The second mRNA problem is that the spike protein is the actual active agent causing damage, in terms of eliciting an immune response. This is the cytokine storm problem that causes the side effects of clotting and of heart failure due to mitochondrial damage. What causes the decreased energy transformation in the patient with side effects? The genetically modified spike protein. Therefore, the range and severity of adverse events potentially attributable to the level of expressed spike protein may reflect patient-to-patient differences due to their individual mitochondrial redox variability in genetic transfer efficiency and subsequent spike expression.
You might want to read this after the blog is assimilated as well. The perspective will fill out your understanding of what is really going on with censorship in science today. HYPERLINK
Natural genetic modification by the immune system to a pathogen is done with finesse and precision by our cell-mediated and innate immune arms themselves, without damaging the mitochondrial genome. In contrast, artificial genetic modification done in the laboratory by genetic engineers is crude, imprecise, uncontrollable, and ends up scrambling and damaging the mitochondrial genome with totally unpredictable effects on safety based upon what was translated from the mRNA. It also interferes inevitably with the natural genetic modification process, and that is ultimately why artificial genetic modification is inherently hazardous.
What can the average citizen do to get involved in the genetically modified vaccine debate?
Take it upon yourself to understand the science behind genetic engineering, expose the lies and half-truths you’ve been told; that’s how to learn real science, and it is fun. That is why you sign up here to be my patron. Don’t be intimidated by the ‘experts’. They are paid to shill for Big Pharma.
Life is simply to understand when you understand its wiring diagram.
Our colony of mitochondria is the primary producers of the body’s energy, mutations in their DNA alters the myriad of energy transformations that lead to size and shape changes inside of cells because altered energy levels cause the DNA to change their transcription of proteins and it is these small changes inside of cells that cause most human disease.
The idea is simple but has alluded modern medicine because of their Dunning Kruger moment of never realizing that the physics of organisms is all about energy transformations.
Space tells matter how to move and matter tells space how to curve and light follows this curve in space. Nature uses a science so queer to innovate living things which always causes outrage in physicians because it offends the common sense of the history medicine.
Waves do not describe a ‘real’ microworld but waves provide us ‘knowledge’ of how energy is traveling through spacetime and that is useful for making predictions in Nature
Humans who abuse technology perceive their world like they have an exemption from the competition of natural selection. They don’t. This paper in the hyperlink below explains it simply.
All of nature is a battlefield.
Life is just a series of wave forms that collides with matter after space has moved it.
Life is just the history we pay attention too, the rest is just the packaging. Change your focus and awareness you change your life.
Well, well the mainstream is catching up and Dr. Wallace getting his due. Now, when they realize the link between light, circadian biology, and mitochondrial function, then they can talk about the prevention/reversal of chronic disease. HYPERLINK
CITES:
1. Shpilka, T. & Haynes, C. M. Nature Rev. Mol. Cell Biol. 19, 109–120 (2018).
2. Guo, X. et al.Nature 579, 427–432 (2020).
3. Tigano, M., Vargas, D. C., Tremblay-Belzile, S., Fu, Y. & Sfeir, A. Nature591, 477–481 (2021).
4. McArthur, K. et al.Science 359, eaao6047 (2018).
5. White, M. J. et al.Cell 159, 1549–1562 (2014).
6. West, A. P. et al.Nature 520, 553–557 (2015).
7. Dhir, A. et al.Nature 560, 238–242 (2018).
8. Majoros, A. et al.Front. Immunol. 8, 29 (2017).
9. Alexeyev, M., Shokolenko, I., Wilson, G. & LeDoux, S. Cold Spring Harb. Perspect. Biol. 5, a012641 (2013).
10. Rehwinkel, J. & Gack, M. U. Nature Rev. Immunol. 20, 537–551 (2020).
11. Borowski, L. S., Dziembowski, A., Hejnowicz, M. S., Stepien, P. P. & Szczesny, R. J. Nucleic Acids Res. 41, 1223–1240 (2013).
You are about to dive into a story that, for quite some time now, has been nothing but a great-sounding idea — a wonderful “what if.” Almost nothing of this story could be found in the mainstream media.
However, the bizarre origin of the story did briefly find its way into FOX’s Glenn Beck show in 2009 as the video above shows you.
I highly recommend you watch this first, as it will draw you directly into the mystery — which flickered for the briefest moment in mainstream media, only to disappear into shuddering silence.
Notice that Beck says FOX contacted the Treasury Department about this case, and received an official blow-off letter in response — basically saying they had “no comment” on this 134 billion dollars in US bonds, seized at the Italian border, as it was “evidence in an ongoing investigation.”
Beck then goes on to put up the numbers of which countries hold the largest numbers of US bonds. In order, they are China at 763.5 billion, Japan at 685.9 billion, the United Kingdom at 152.8 billion, Russia at 137.0 billion and Brazil at 126.0 billion.
Based on the public, unclassified numbers, 134.5 billion dollars in US bonds could only have been produced by Russia, the UK, Japan or China… no one else. The amount of money is so huge that if Russia produced it, they would only have 2.5 billion dollars in US bonds left over!
Joe Wiesenthal, the editor of BusinessInsider.com, said that whether this was a government dumping its bonds or a counterfeit operation, it was “gigantic” in scope and “unlike anything we’ve ever seen — not just in size but also in sophistication.”
According to Wiesenthal, in order to counterfeit these bonds, “it would be the kind of technology you would expect only a government to have.” Wiesenthal also believes the 1934 issuance date on the bonds suggests they may be elaborate forgeries. Bonds are just like money in the Federal Reserve legacy system. Who has more bond assets than any other company right now in the world?
BLACKROCK.
If the name BlackRock sounds familiar as of late, that is because this entity is also gobbling up real estate, usually at well over the asking price. This is a big reason why real estate prices are the highest they have ever been along with asset inflation by QE from their partners at the Federal Reserve
This plan is laid out by the WEF books linked to Schwab’s Fourth Industrial Revolution. Read these books to see how the families control the pieces on the monopoly board. Why do they lay the plan out for all to see? To show you how powerful they really are. It is akin to a bond thief who counterfeits the bonds artwork and leaves his signature camouflaged in his masterpiece to let the world know how much smarter they are than anyone else. This is wealth redistribution 101, and it isn’t a financial derivative where the rich people’s wealth is getting redistributed.
What will make 82 million people in the future sell their house to Blackrock, Vanguard, whoever, you ask?
That is the wrong question to ask. The WEF has a different plan.
This is the fundamental misunderstanding professional market analysts are making on this. They dont have to force anyone to sell. They just have to buy enough new homes for the next 10 or 20 years that it becomes exceedingly difficult for new buyers to enter the market. It’s a long play that the WEF is interested in.
By 2028, BlackRock and Vanguard will own almost everything in many asset classes, which is the stated goal of the WEF in all their books. You should go read some of them to see if I am lying to you. Ideation without execution leads to deletion of every good idea. BlackRock and Vanguard are the executioners of WEF plans in today’s investing world. None of them want you to know about much less own any Bitcoin. Owning BTC is an impediment to their plan. Why?
The angle of attack of the WEF is to make sure the price of a home is out of your reach and they will sociall engineer you into being a life long renter. You’ll look into your mirror everyday and say, “how can I afford a house? You won’t be able too. That is the goal. Those homes Black Rock is scooping up today, in 2-3 decades will be 20, 30 yrs old: at best by the time a current 5th grader is, say 30 yrs old. And he won’t likely be offering what the market wants when he is 30, namely 30-40% down.
Don’t be fooled into thinking they need to court people who will be 50-70 yrs old, and home owners in 2030, 2040, 2050. They’ll have stymied enough of those under 30 years old from building enough wealth to be capable of buying a home. They’ll need 120k or 150k down just to compete in the future market place, and they wont have it, by social engineering design, and this will keep everyone as a renter/slave to the property owner. They will be slaves to BlackRock just to have a place to live. That is the goal of the WEF. You’ll own nothing and be happy about it.
With 10-20 years of this BlockRock buy up you’ll see a perceptual shift in future generations or home ownership. It has already happened to millennials. Owning a home won’t have been a wealth generating tool for a decade or more in 2030. Moreover, the kids of today won’t even see a home as an asset to build wealth. Instead, through financial engineering, they’ll view it as an albatross. So the impetus to own a home won’t be there the way it was 20 years ago or even today. That is the goal. To change their perceptions of how to do wealth and make sure they remain financially illiterate. This is why BTC ownership is critical to the younger generations of today, and few of the know it.
It’s similar to how those today who are under 25 don’t have a recognition of living in a pre-9/11 world. They don’t really know what that means or entails. They’ve only known a post-9/11 existence and that existence is dominated by the catastrophe 2008 had on their parents. It will be the same with home ownership, if localities don’t stop major investment firms current practices of buying up neighborhoods, the WEF’s goal is a one world government with one currency, they make the rules of how you live.
Bitcoin will allow you to be a divergent in this world. You should not, and cannot fear Bitcoin right now. That is why when it dips today, you better buy it and not fear their FUD creation. They are hoping to scare you so you never buy your freedom card again.
To be afraid, is to prepare one’s self to obey a master.
Decide that you want it more than you are afraid of it.
If you want to control someone, all you have to do is to make them feel afraid.
Inaction breeds doubt and fear. Action breeds confidence and courage.
If you want to conquer fear, do not sit home and think about it. Go out and get busy and do something productive
Fear keeps us focused on the past or worried about the future. If we can acknowledge our fear in the now, everything becomes crystal clear.
Today, for BlackRock and Vanguard borrowing money is dirt cheap to buy up assets. This is why they are gobbling up real estate, usually at well over the asking price. This is a big reason why real estate prices are the highest they have ever been along with asset inflation by QE from their partners at the Federal Reserve. Devalued money & bonds today are buying hard assets today, because post economic reset they know the majority of the public will never have the ability to own a house ever again. They want to create a nation of renters.
This plan is laid out by the WEF books linked to Schwab’s Fourth Industrial Revolution. Read these books to see how the families who make up Octagon who control the Bank of International Settlements (BIS) which in turn, controls the Federal Reserve who help move the pieces on the monopoly board to help those families steal wealth of 8 billion people slowly over time below their ability to perceive it.
Why do they lay the plan out for all to see? To show you how powerful they really are. It is akin to a bond thief who counterfeits the bonds artwork and leaves his signature camouflaged in his masterpiece to let the world know how much smarter they are than anyone else. This is wealth redistribution 101, and it isn’t a financial derivative where the rich people’s wealth is getting redistributed right in front of your eyes.
It’s normal American middle class, salt of the earth wealth heading into the hands of the world’s most powerful entities and individuals by financial engineering of the rules of the game. The traditional financial vehicle is gone forever because of how BlackRock, State Street, and Vanguard operate.
If you have ever wondered why television “news” is constantly interrupted by advertising for the latest drug offerings from Big Pharma, look no further than Blackrock and Vanguard, two of the world’s largest asset management companies, which just so happen to own both the drug industry and the media.
BlackRock and Vanguard are currently the top two owners of Time Warner, Comcast, Disney, and News Corp. These four media conglomerates own and control more than 90 percent of the United States media landscape, which explains why their collective coverage of world events all centers around the same propaganda.
Though most people have never heard of them, BlackRock and Vanguard are also the silent monopoly owners of many other facets of the economy. They are said to hold ownership in some 1,600 American firms which, as of 2015, held combined revenues of $9.1 trillion. The number is now over 30 Trillion in 2021.
CHINA’S DRAGON FAMILIES ARE NOT WHO YOU THINK THEY ARE
When you understand the Chinese BTC miners represent the Chinese elder families who had their gold stolen from the families who own the US Fed, you understand that the BTC miners in China are not CCP friendly and abhor the US bankers. You also begin to understand why the Chinese elder families want to replace their metallic gold with digital gold and why the CCP is cracking down on BTC miners right now.
The Chinese Elders sued the Federal Reserve families in September 2010 for gold contracts going back hundreds of years, in a secret world court within the BIS — and the Elders won as of December 2020. This lawsuit has a lot to do with Bitcoin’s future. Where did this lawsuit begin?
Ever since this bizarre event happened in the hyperlink, the only follow-up to the story has been in the form of an elaborate amount of ‘insider’ information leaked by Benjamin Fulford — the former Asia-Pacific bureau chief for Forbes Magazine — on a week-by-week basis. The video above was the giant rabbit hole I jumped down to solve this mystery. Here is his media page.
Finally, the lawsuit at the epicenter of this investigation has now become a tangible reality — validating everything Fulford has been saying about this mysterious case since it originally started.
Looming storm clouds threatened to demolish Fulford’s credibility in a single crash of lightning as the all-important date of November 15th, 2011 came and went — with nothing to show for it — after years of fanfare and buildup on his financial websites.
However, on November 23, 2011, the clouds parted. A vast, 111-page legal complaint was filed in the United States District Court for the Southern District of New York. This complaint is now a provable matter of public record… as you are about to see.
GO LOOK FOR YOURSELF
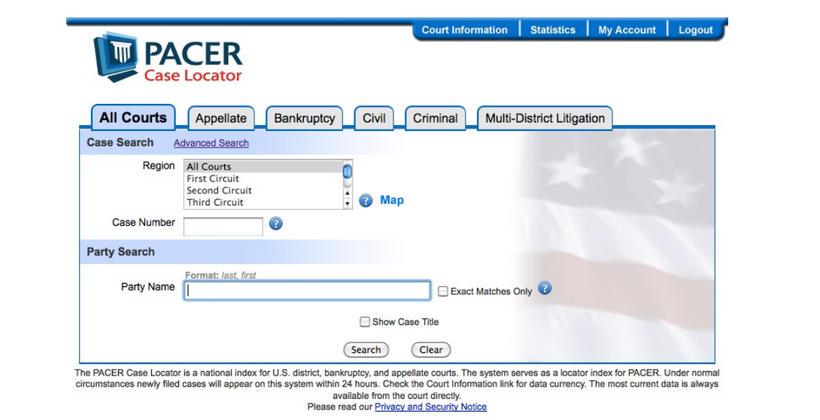
Here is the search window that opens up when you go to pacer.gov and register as a user for eight cents a page. This website is a public service that allows you to search for any and all legal cases that have been filed in America:
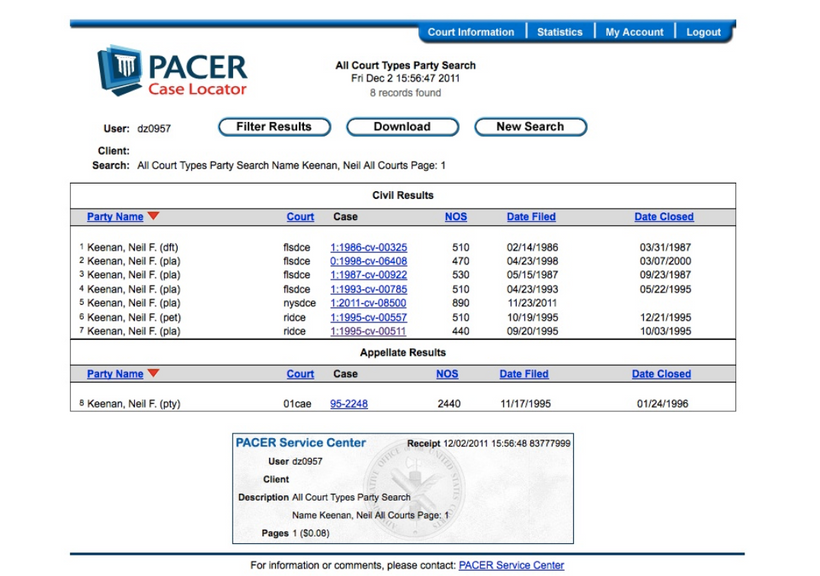
Once you’ve set up your user account, type in “Keenan, Neil” under “Party Name”, and you will then see this:
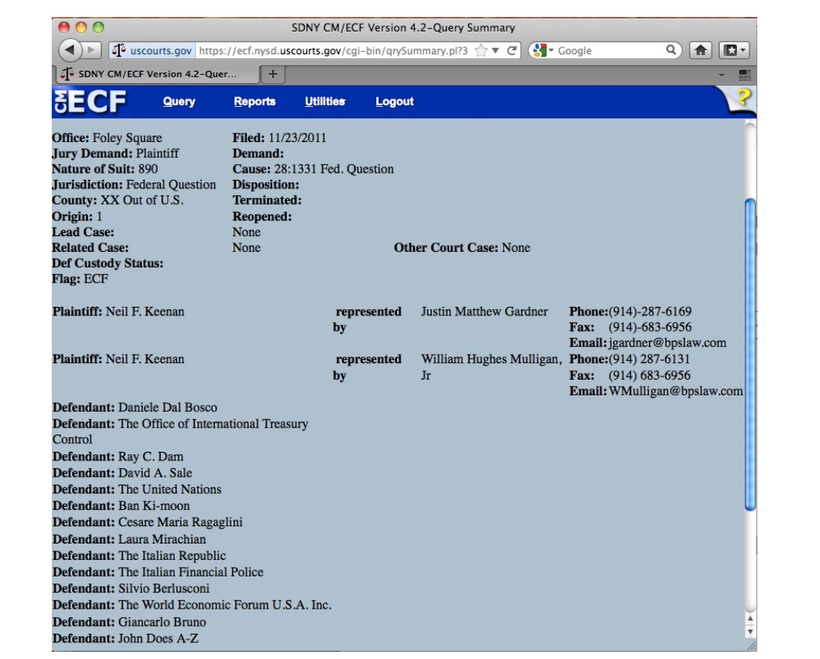
Notice the fifth item down on the list… 2011-cv-8500, filed on November 23, 2011. That’s the one. You can then click into it from there, and one of the screens you will pull up is the following:
Did you catch that list of defendants above?
If the amount of money being sued for isn’t stunning enough, that list of defendants should attract a great deal of attention — for it includes the Italian Republic, the Italian Financial Police, Italy’s Prime Minister Silvio Berlusconi, the World Economic Forum, Ban Ki-Moon (the old head of the UN), and the United Nations itself.
What the hell is going on here you ask????
If you don’t want creepy government spies watching you, and you don’t want to pay eight cents a page, here’s the entire PDF file as it appears once you download it off the PACER website: HYPERLINK
MAINSTREAM MEDIA PICKED UP THE STORY AS OF DECEMBER 5, 2011
Dan McCue started asking the same questions you may now be thinking about… and as a result, he was the first mainstream journalist to cover this story in Courthouse News Service, a nationwide news service for lawyers and the news media.
McCue isn’t necessarily convinced — the article is entitled “Bizarre Claim for $1 Trillion” — but given that this is a real case, he is certainly interested enough to write about it.
THE FIRST MAINSTREAM ARTICLE TO EXPLORE THIS STUNNING CASE
MANHATTAN (CN) – An American expatriate in Bulgaria claims the United Nations, the World Economic Forum, the Office of International Treasury Control and the Italian government conspired with a host of others to steal more than $1.1 trillion in financial instruments intended to support humanitarian purposes.
The 111-page federal complaint involves a range of entities common to conspiracy theorists, including the Vatican Illuminati, the Masons, the “Trilateral Trillenium Tripartite Gold Commission,” and the U.S. Federal Reserve.
Plaintiff Neil Keenan claims he was entrusted in 2009 with the financial instruments — which included U.S. Federal Reserve notes worth $124.5 billion, two Japanese government bonds with a combined face value of $19 billion, and one U.S. “Kennedy” bond with a face value of $1 billion — by an entity called the Dragon Family, which is a group of several wealthy and secretive Asian families.
“The Dragon family abstains from public view and knowledge, but, upon information and belief, acts for the good and better benefit of the world in constant coordination with higher levels of global financial organizations, in particular, the Federal Reserve System,” Keenan claims.
“During the course of its existence over the last century, the Dragon family has accumulated great wealth by having provided the Federal Reserve Bank and the United States Government with asset assignments of gold and silver via certain accounts held in Switzerland, for which it has received consideration in the form of a variety of Notes, Bonds and Certificates such as those described … that are an obligation of the Federal Reserve System.”
Keenan says that with accrued interest the instruments are now worth more than $1 trillion. He says the family designated him as its principal in an effort to select certain registered and authorized Private Placement Investment Programs (PPPs) for the benefit of unspecified global humanitarian efforts.
In his remarkable complaint, Keenan claims that the U.S. government [received] enormous amounts of money — delivered in gold and other precious metals — from the Dragon Family many years ago, and that the money was placed into the Federal Reserve System for the benefit and underwriting support of the dollar, “which was to become and currently remains the global reserve currency”….
The complaint alleges a complicated history with many moving parts and scores of internationally known and unknown characters, the sum of which is that Keenan claims he was entrusted with billions of dollars in bonds by the Dragon Family….
These instruments were then stolen as two Japanese agents attempted to cross the border from Italy into Switzerland with them, contained in the suitcase. It has taken me years to find the names of the agents. One was named Satoshi Yamamoto and the other was named Nakamoto Haruto. That find stunned me. Why?
In Japan, like in China and Korea, the first name follows the family name. A person with the first name “Ichiro” and the family name “Suzuki” is, therefore, called “Suzuki Ichiro” rather than “Ichiro Suzuki”.
What is the pseudonymous name of linked to the Bitcoin White paper?
[Keenan] claims that as the conspiracy continued to unfold, various high level officials repeatedly offered him a bribe of $100 million to “release” the instruments without disclosing their theft to the Dragon family, and to allow the instruments to be converted to a so-called UN “Sovereign Program” wholly under the auspices, protection and umbrella of the sovereign immunity enjoyed by the defendants.
Other defendants include UN General Secretary Ban Ki-Moon, Former Italian Prime Minister Silvio Berlusconi, Giancarlo Bruno, who is identified as head of the banking industry for the World Economic Forum, Italy’s ambassador to the UN Cesare Maria Ragaflini, Ray C. Dam, president of the Office of International Treasury Control, and David A. Sale, the deputy chief of the council for the cabinet of the OITC in 2011.
Keenan seeks the return of the stolen instruments, punitive damages and court costs on multiple claims of fraud, breach of contract and violation of international law.
He is represented by William H. Mulligan Jr., with Bleakley, Platt & Schmidt of White Plains, N.Y.
Unfortunately Courthouse News Service, website was removed by the FBI from the web for some unknown reason years ago. McCue did a great job of summarizing the rest of the case on that site but it is lost forever now. This is just an overview of what was on that site when it was live.
YOU HAVE GOT TO BE KIDDING ME FILE
Courthouse News Service didn’t quite have the stomach to quote one of the most interesting paragraphs in the entire complaint… but I do. This is where the whole story really started taking shape for me:
Thousands of trillions of dollars? You have GOT to be kidding me! As soon as I read that, I had to know more… because I had enough information to be convinced that this was not a spurious lawsuit. I emailed Fulford to try to educate myself and was sent down a few rabbit holes.
Neil Keenan, the principal plaintiff in this case above, as well as Keith Scott, who is also mentioned in the complaint. Scott is an expert in this utterly secretive world of trading between central banks — and is well aware of the vast wealth underwriting them, all held in the strictest secrecy.
Keenan has never worked for any government or clandestine agency. He is a businessman who ultimately became acquainted with the Dragon Family — the former ruling party of China, prior to the arrival of Communism — and gained their trust.
WHO ARE THE DRAGON FAMILY?
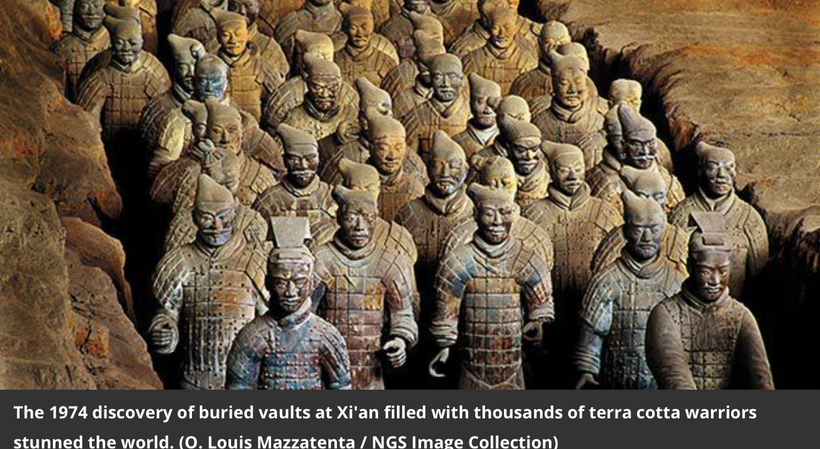
In March 1974, a group of peasants digging a well in drought-parched Shaanxi province in northwest China unearthed fragments of a clay figure—the first evidence of what would turn out to be one of the greatest archaeological discoveries of modern times. Near the unexcavated tomb of Qin Shi Huangdi—who had proclaimed himself first emperor of China in 221 B.C.—lay an extraordinary underground treasure: an entire army of life-size terra cotta soldiers and horses, interred for more than 2,000 years.
China was named after emperor Qin, the first ruler in the Dragon Family. That was the first dynasty of China. Qin was the ruler who built the Terra Cotta Soldiers, where he took every soldier and every horse in his army and built a stone sculpture out of them and buried them in a mountain. There’s all sorts of interesting historical facts about how this Dragon family showed up. Much of what they do mimics what Micheal Burry does with his tweets. They basically erased all the history from China before they existed, which is now being rebuilt by certain scholars. Apparently, that is how the ancients remained clandestine because back then communication was limited and this kept their enemies in the dark about their true intentions. These Asian secret societies appear to be dynastic. They’ve largely been behind the scenes. They’ve amassed large amounts of wealth. This wealth was used to Fund the Federal reserve in 1913. That gold was stolen from them when the USA military became powerful and the USA stole the gold via their judicial system. The Dragon family then came up with a plan to level the playing field. THE DRAGON FAMILIES WANT A FAIRER SYSTEM, NOT DOMINATED BY THE WEST
They think that the control of the future of the planet should no longer be controlled by a small Western elite. They would rather have it fall under the control of the people of the planet.
BIS WANTS CENTRAL CONTROL of money. This is their headquarters above. Who is BIS? BIS was founded by four men on 5/17/1930,: Hjalmar Schacht [Head of Reichsbank], Charles G Dawes [Chairman of City National Bank], Owen D Young [founder of RCA and chairman of General Electric] and Montague Norman [governor of the Bank of England and partner in JP Morgan]. Now you can see the tentacles of this tribe.
From the founding of the bank (BIS) until at least 1939, Schacht worked closely with Jacob Schiff, the Warburgs and Montague Norman, in funneling Wall Street and City of London money into Hitler’s rearmament program; as is documented in Professor Antony Sutton’s painstaking work, Wall Street and the Rise of Hitler:
“In October 1931, Warburg received a letter from Hitler which he passed on to Carter at Guaranty Trust Company, and subsequently another bankers’ meeting was called at the Guaranty Trust Company offices. Opinions at this meeting were divided. “Sidney Warburg” reported that Rockefeller, Carter, and McBean were for Hitler, while the other financiers were uncertain.
Montague Norman of the Bank of England and Glean of Royal Dutch Shell argued that the $10 million already spent on Hitler was too much, that Hitler would never act. The meeting finally agreed in principle to assist Hitler further, and Warburg again undertook a courier assignment and went back to Germany.
On this trip Warburg reportedly discussed German affairs with “a Jewish banker” in Hamburg, with an industrial magnate, and other Hitler supporters.
One meeting was with banker von Heydt and a “Luetgebrunn.” The latter stated that the Nazi storm troopers were incompletely equipped and the S.S. badly needed machine guns, revolvers, and carbines.”
This evidence shows that the transfers of those funds into the accounts held in trust by BIS for Hitler’s regime were all facilitated by the Warburgs, a family which long ago assimilated itself into the House of Rothschild by marriage and without whom the Rothschild’s hand in world affairs would not have been capable of remaining hidden for so long.
It is therefore fair to deduce from this circumstantial evidence alone that the Warburgs were acting as Rothschild proxies in the financing of Hitler’s rise to power, in which they were aided and abetted by at least two of the four BIS founders, in Schacht and Norman.
WHY IS THIS IMPORTANT TODAY?
The US Federal Reserve is linked to BIS in cornerstone fashion.
Paul Warburg was also the driving force behind the creation of the US Federal Reserve, which congressman Charles Lindbergh described as: “…the most gigantic trust on earth. When the President [Wilson] signs this Bill, the invisible government of the monetary power will be legalized… The greatest crime of the ages is perpetrated by this banking and currency bill.”
That is how your Fed links to the BIS and the Octagon families.
Why is China’s CCP dumping all things bitcoin right now?
Did you know that a key CCP official defected to the USA recently? He turned himself over to the DIA (defense intelligence agency). Guess why he chose them? Minister Dong Jingwei choose to defect to the Defense Intelligence Agency and not the CIA or NSA like usual. That makes this an industrial military game who protects the BIS or Federal bankers.……….yet.
Who is this guy?
Minister Jingwei was a Counterintelligence Boss, essentially the Chief Spy Catcher of the CCP. His job was to ensure that Spies in China or working overseas against Chinese Interests were caught. He is part of the Dragon family ancestry.
Many of the spies were linked to Wuhan Institute and the CBDC/digital yuan rollout plans.
He was in charge of surveillance capitalism, the take over of Taiwan, and Diego Garcia in the Indian Ocean. (BTC #4 blog)
The bottom line is that the Chinese Dragon Family intended for these bonds to be stolen to set legal precedent in the Old World Court system.
They represented only a small percentage of the overall asset base… all of which is clandestinely registered within the Federal Reserve and the Bank of International Settlements in Basel!
This was an elaborate sting operation that has brought us to where we are today in financial markets — where a vast international alliance of 117 countries now has a legal way to end the financial tyranny of the Old World Order (WEF) that the families I mentioned above have been forcing on the rest of the world through their action arms like BlackRock and Vanguard.
Might the 1 million coins on BTC blockchain that have not been touched ever be owned by the Chinese Dragon Families? Might the Japanese name of Satoshi Nakamoto have particular relevance to this story laid out above? I think it might. I think the battle over the New World Order and Old World Order is linked to this lawsuit in the Southern District of New York, and why Central bankers all over the world abhor Bitcoin.
A STAGGERING AMOUNT OF INFORMATION IS BURIED FROM US.
In truth, BlackRock and Vanguard are one and the same entity, seeing as how the latter is the largest shareholder of the former. Among the family names tied into the two are the Freemasons and the P2 Lodge,Rothschilds, the Bushes, the British Royal family, the Du Ponts, the Vanderbilts, and the Rockefellers. These families have created Bezos and Elon Musk to help faciltate the wealth redistribution on their behalf. Be careful who you worship and adore because they maybe be your “Brutus” tomorrow. These families make up the Octagon network that control the BIS now.
The Chinese triads, the Japanese yakuza groups and various other secret groups in Asia have strict rules against nepotism. This is another reason the Dragon families are at war with the groups above. All of them favor nepotism as a means of generational control.
BLOCKROCK OWNS THE MEDIA. The media is the entertainment division of the industrial military complex to keep things running smoothly during the Economic Reset.
All of these families have been pushing for a New World Order for centuries, and it would appear as though they are on the verge of achieving their goal through the destruction of world financial systems, the gobbling up of all real estate, and eventually the total abolition of private property. Klaus Schwab, George Soros, and Henry Kissinger are the living spokesmen of this Old World centralized empire.
Nixon protected the people who formed and now own BlackRock. BlackRock is part of the Octagon network that links the Fed and the WEF. The BUSH family is a major stakeholder in Black Rock and they have deep ties to the CIA and FBI through positions their family have held in government. George H Bush was the president in 2011. https://thestrategystory.com/2020/09/18/blackrock-shadow-bank/
Robert Mueller……….remember him. “Independent council “formerly head man at the FBI. How independent can you be when you are investing your own department for misconduct? See how the WEF operates? They control the fox allowed into the hen house so they cannot lose.
What this means is that BlackRock/Vanguard together own pretty much everything there is to own, which explains why everything is now moving in one general direction, straight towards an economic reset. No matter the industry or the sector, BlackRock and Vanguard more than likely hold a stake and control the movement.
The stock of the world’s largest corporations is owned by the same institutional investors. They all own each other. This means that ‘competing’ brands, like Coke and Pepsi or NBC and Fox, aren’t really competitors, at all, since their stock is owned by exactly the same investment companies, investment funds, insurance companies, banks (see their tweet below), and in some cases, governments. The media is the entertainment division of BlackRock’s military division.
That is your reality now. You cannot trust anyone but yourself to make the right call for you and your loved ones.
SUMMARY:
Warburg’s reward for bringing into being the U.S. Federal Reserve was to be its first chairman. While speaking before the House Committee on Banking and Currency in 1913, he confessed that, having emigrated to America in 1902, following an extensive education in international banking in Europe, he became a partner of Kuhn, Loeb & Co, which was to become a Rothschild-controlled shareholder of the American central bank.
It is self-evident that the education Warburg received was given by the Rothschilds, just as it was given to Jacob Schiff whilst he lived at their Frankfurt home before emigrating to America.
Between the American Civil War and the beginning of the First World War, the main U.S. agents of the Rothschild Empire were JP Morgan, Abraham Kuhn and Solomon Loeb. Newsweek magazine published a brief history of Kuhn, Loeb & Co on February 1st 1936, which stated:
“Abraham Kuhn and Solomon Loeb were general merchandise merchants in Lafayette, Indiana, in 1850. As usual in newly settled regions, most transactions were on credit. They soon found out that they were bankers…
In 1867, they established Kuhn, Loeb and Co., bankers, in New York City, and took in a young German immigrant, Jacob Schiff, as partner. Young Schiff had important financial connections in Europe.
After ten years, Jacob Schiff was head of Kuhn, Loeb and Co., Kuhn having retired. Under Schiff’s guidance, the house brought European capital into contact with American industry.”
Those European “financial connections” were the Rothschilds, in whose Frankfurt house Jacob Schiff was purportedly educated; and their German partners, the M.M. Warburg Company of Hamburg and Amsterdam, who were and remain but an extension of the same all-powerful banking house – Rothschild by another name.
During the latter decades of the previous century, the Rothschilds provided John D. Rockefeller with enough finance to develop and dramatically expand his Standard Oil business which was broken up and whose fragments became modern day Big Pharma, Oil, and chemical empires.The mechanics of the investment were performed by the Warburgs and Jacob Schiff at Kuhn Loeb, who also financed Edward Harriman’s and Andrew Carnegie’s rail-road and steel empires;whilst JP Morgan’s empire was founded on credit extended by the Rothschild-controlled bank in New York.
Those of you who are full members of my website should go back and revist the webinar (Aug/Sept 2018) I did on the three robber barrons and how they ruined modern medicine with the Flexner report.
It naturally follows that, on the basis that the names of Warburg, Morgan and Schiff are synonymous with that of Rothschild, the banking house is widely considered to have power, control or undue influence over every member of the Federal Reserve board, as well as the selection of its chairman.
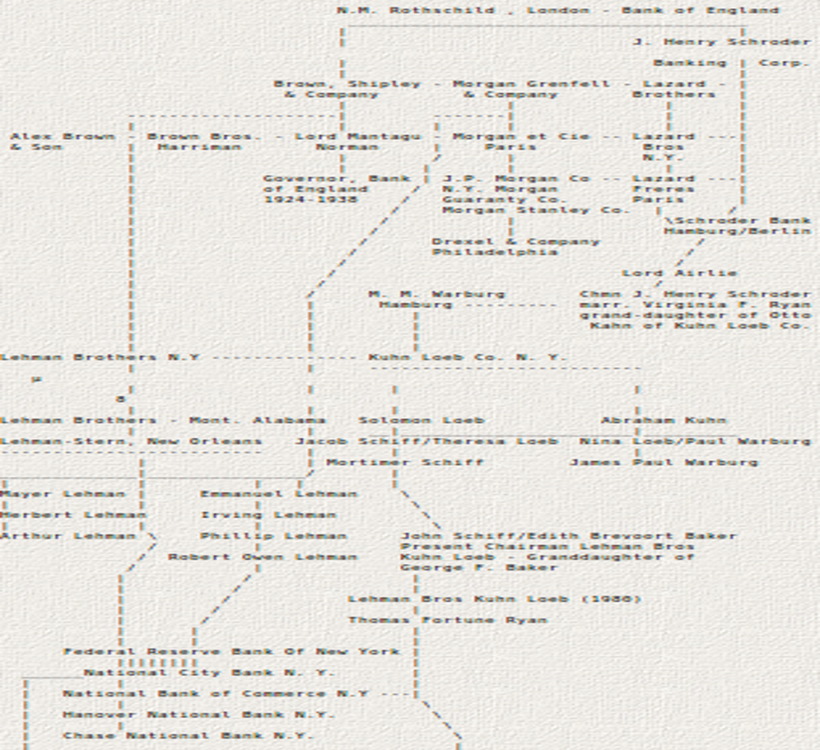
In August 1976, the House Banking Committee Staff Report was published, detailing the history of the board members of the Federal Reserve, a portion of which can be seen below:
I’m sorry this picture is not ideal but that is what we have left in archives. In the event this table is accurate [and there is no reason to believe it is not based on my research], there is not one individual or bank or investment company included that could not be considered a Rothschild interest, whether by partnership, investment, lending, commissioning or founding, at the time the Federal Reserve Act was passed into law.
IT GETS WORSE
Reflecting upon the 1907 panic, Paul Warburg, when speaking to the Banking and Currency Committee, confirmed that he was a driving force behind the Aldrich Plan for the creation of a privately owned US central bank:
“In the Panic of 1907, the first suggestion I made was, “let us have a national clearing house” [Central Bank]. The Aldrich Plan [for a Central Bank] contains many things that are simply fundamental rules of banking. Your aim must be the same.”
In addition to this compelling evidence of the hidden hand of Rothschild influence and control, the Telegraph newspaper published an article on 31/07/2013, detailing the revelations contained in documents released by the Bank of England, concerning the transfer of Czech gold to the Reichsbank BIS account. The article stated:
“The documents reveal a shocking story: just six months before Britain went to war with Nazi Germany, the Bank of England willingly handed over £5.6 million worth of gold to Hitler – and it belonged to another country.
The official history of the bank, written in 1950 but posted online for the first time in 2018, reveals how the BRITS betrayed Czechoslovakia in WW2 – not just with the infamous Munich agreement of September 1938 (Chamberlin), which allowed the Nazis to annex the Sudetenland, but also in London, where Montague Norman, the eccentric but ruthless governor of the Bank of England agreed to surrender gold owned by the National Bank of Czechoslovakia to Hitler. Still think a centralized system is not a problem?
The Czechoslovak gold was held in London in a sub-account in the name of the Bank for International Settlements, the Basel-based bank for central banks. When the Nazis marched into Prague in March 1939 they immediately sent armed soldiers to the offices of the National Bank. The Czech directors were ordered, on pain of death, to send two transfer requests.
The first instructed the BIS to transfer 23.1 metric tons of gold from the Czechoslovak BIS account, held at the Bank of England, to the Reichsbank BIS account, also held at Threadneedle Street.
The second order instructed the Bank of England to transfer almost 27 metric tons of gold held in the National Bank of Czechoslovakia’s own name to the BIS’s gold account at the Bank of England.”
To get more information on history of the Fed and BIS read cite one below.
WAS COVID ANOTHER CZECH GOLD STEAL?
COVID was a compliance test for the economic reset upon us. The WEF Octagon families own all of Big Pharma.
For a virus with a survivability rate of 99.8%, the West imploded upon itself and destroyed all resemblance of liberty in less than two weeks. Now it recommends a manufactured solution brought to you by the families who are controlled by the WEF. Amazing coincidence. Imagine if we had a real, sudden extensional emergency and crisis on our hands. What would stupid thinking humans default then? Twitter?
Who controls the media and what have they told us?
BlackRock, Vanguard, and WEF control NBC. The WEF controls the CDC & WHO. The Federal Reserve instituted lockdowns because the CCP asked the world to do that. This is how you engineer a wealth transfer upon obedient idiots. (technocracy link)
The Soviet Union tried to beat the west. Xi Jinping simply bought it using ads on MSM. The WEF and WHO and CDC all helped set it up. Don’t believe it yet?
The Chinese Communist Party Hid Vital Information from the World and the World Health Organization Chose to Placate Rather Than Act, Allowing the Virus to Spread Globally
December 2019 – January 2020: CCP leaders know about coronavirus, but take aggressive steps to hide it from the public, including detaining doctors who warned about the virus and censoring media on the virus.
Dec. 30, 2019: Doctors in Wuhan report positive tests for “SARS Coronavirus” to Wuhan health officials. Under WHO regulations, China is required to report these results within 24 hours. China fails to inform the WHO about the outbreak.
Dec 31, 2019: WHO officials in Geneva become aware of media reports regarding an outbreak in Wuhan and directs the WHO China Country Office to investigate. Taiwan informs WHO about human-to-human transmission, but data is not published on WHO’s data exchange platform.
Jan 1, 2020: Hubei Provincial Health Commission official orders gene sequencing companies and labs who had already determined the novel virus was similar to SARS to stop testing and to destroy existing samples.
Jan 2, 2020: The Wuhan Institute of Virology (WIV) completes gene sequencing of the virus, but the CCP does not share the sequence or inform the WHO.
Jan 3, 2020: China’s National Health Commission ordered institutions not to publish any information related to the “unknown disease” and ordered labs to transfer samples to CCP controlled national institutions or destroy them.
Mid-Late January: Despite knowing about the virus, CCP allowed massive travel within China and abroad during the Spring Festival (3 billion estimated trips over 40 days), and Wuhan held a celebratory potluck with more than 40,000 families eating from 14,000 dishes
Jan 11-12, 2020: After a researcher in Shanghai leaks the gene sequence online, the CCP transmits the WIV’s gene sequencing information to the WHO that was completed 10 days earlier. The Shanghai lab where the researcher works is ordered to close.
Jan 14, 2020: Wuhan health authorities claim no human to human transmission from coronavirus. This assessment was tweeted by WHO the same day. According to classified documents obtained by the Associated Press, Xi Jinping is warned by top Chinese health official that a pandemic is occurring. He did not care because he has full control of the West’s media by way of the WEF. The WEF and the CCP now have deep influence in Washington DC because the FBI and CIA helped them gain power in the last election of President.
Jan 22, 2020: WHO mission to China admits some evidence of human-to-human transmission.
Jan 23, 2020: After the Emergency Committee is divided on whether to declare a Public Health Emergency of International Concern (PHEIC), Director-General Tedros decides not to. This delay contributed to a regional epidemic turning into a pandemic
Jan 23, 2020: The CCP institutes a city-wide lockdown of Wuhan. However, before the lockdown goes into effect, an estimated 5 million people leave the city. Lockdowns do not work for coronavirus but they are quite good at shutting down an economy.
Jan 29, 2020: Tedros of the WHO praises the CCP’s response to the virus, saying their transparency was “very impressive, and beyond words” and that the CCP was “actually setting a new standard for outbreak response.” LOL
Jan 30, 2020: One week after declining to do so, Tedros declares a Public Health Emergency of International Concern. LOL
Feb 16, 2020: WHO and PRC officials begin a nine-day “WHO-China Joint Mission on Coronavirus Disease 2019” and travel to China to examine the outbreak and origin of COVID-19. Many team members, including at least one American, were not allowed to visit Wuhan on the trip.
March 11, 2020: The WHO officially declares the COVID-19 outbreak a pandemic after 114 countries had already reported 118,000 cases including more than 1,000 in the United States.
If you do not think all three branches of government are compromised then you must have missed this news below from the SCOTUS this week about slavery.
The Declaration of Independence says, “It is the right of the people to alter or abolish” a government deemed to be abusive by the governed. We are getting closer to that reality. I see a legal case developing now in the world around us. We have allowed the government and its agents too much power in controlling our lives.
The answer: Buy a lot of BTC. They will create FUD to keep you afraid of buying it. Do not stop filling your life raft. You life might soon depend on thinking critically. Don’t buy any BTC via a phone device and never store it on a phone wallet.
Bitcoin is a hard fork of gold. A needed system upgrade to ensure state resistance and decentralization. BTC is the vaccine against the plague in power now in the banking system.
Human history is the story of evolution which is a byproduct of entropy. We all still subject to the laws of physics and time. The game is to accumulate and store as much energy as possible. Fiat money is not real money. If you think paper dollars = wealth, then you deserve what is coming.
You will never achieve peace of mind as long as you still have people you cannot trust around.
That is tied to the dopamine levels in the pelvic wall. Women who rarely get their perineum in the sun suffer from this due to altered fiber type in the pelvic muscles as the video above show. This effect is mediated by dopamine changes in the muscles. Dopamine is made by aromatic amino acids which absorb solar energy in the UV range to deliver energy to optimize the function of muscles.
The dopamine system plays an integral role in motor physiology. Dopamine controls movement by modulation of higher-order motor centers (e.g., basal ganglia) but is now now known to also regulate movement by directly controlling motoneuron function. Even though dopamine cells synapse onto motoneurons, which themselves express dopamine receptors, it is unknown whether dopamine modulates skeletal muscle activity. More on that below.
Many women with this condition will also have poor hemoglobin and hematocrit levels and this tells us they deliver poor levels of oxygen to their pelvic floor muscles. What are those implication for these women’s pelvic floor colony of mitochondria?
Mitochondrial cristae density is a better predictor of maximal #oxygen uptake than mitochondrial volume. Nielsen et al. 2017 lays out these mitochondrial effects and your doctor should know why anemia is a symptom that foretells cristae collapse in the muscles of your pelvis to affect sexual dysfunction and bowel and bladder incontinence.
WHAT ARE THE PELVIC FLOOR MUSCLES?
The pelvic floor is a group of muscles that stretch like a hammock from the pubic bone at the front, to the coccyx (tailbone) at the back and from one ischial tuberosity (sitting bone) to the other (side to side).
A female’s pelvic floor muscles support her bladder, bowel and uterus (womb). The openings from these organs (the urethra from the bladder, the vagina from the uterus and the rectum from the bowel) pass through the pelvic floor. The pelvic floor muscles wrap firmly around these passages to help keep them shut.
When the pelvic floor muscles are strong they help prevent:
The pelvic floor muscles also help with sexual sensation during orgasm and function.
Continence issues can affect the bladder, bowel or both. In countries with poor UV light from the sun the amount of women with this disease skyrockets. Different cultures who make it perineal health using natural light taboo also have female populations of with a higher incidents of pelvic wall weakness. For example, incontinence is prevalent in the solar poor UK, with an estimated 14 million adults experiencing urinary incontinence (NHS England, 2018; NHS England, 2015) and over 6.5 million having bowel control problems (Yates, 2017; NHS England, 2015). In women, the most prevalent types of continence problems are:
Stress urinary incontinence, which affects 10-39% of women;
Mixed urinary incontinence, which affects 7.5-25% of women;
Urge incontinence, which affects 1-7% of women (Abrams et al, 2017).
Approximately 10% of all adult women experience urinary leakage at least once weekly and 25-45% experience occasional leakage (Abrams et al, 2017).
How to do pelvic floor muscle exercise using sunlight or PBM
Once you can feel your pelvic floor muscles working, you can start exercising them in the light:
Pelvic floor muscle exercises can be done anywhere – while sitting, standing or lying down in the sun.
Squeeze and draw in the muscles around your anus (back passage) and vagina at the same time. Lift them UP inside. You should have a sense of “lift” each time you squeeze your pelvic floor muscles. Try to hold them strong and tight as you count to 8. Now, let them go and relax. You should have a distinct feeling of “letting go”. If you can’t hold for 8, just hold for as long as you can.
Repeat “squeeze and lift” and let go. It is best to rest for about 8 seconds in between each lift up of the muscles.
Repeat this “squeeze and lift” as many times as you can, up to a limit of 8 to 10 squeezes. This equals one set.
Try to do three sets of 8 to 10 squeezes each day.
I just got a new light unit built that is large enough where one can do this in any environment
While doing pelvic floor muscle training:
keep breathing
only squeeze and lift
do NOT tighten your buttocks
keep your thighs relaxed.
Pelvic floor exercises are most effective when individually tailored and monitored. If you are not sure that you are doing the squeezes right, or if you do not see a change in symptoms after three months, ask for help from your family doctor, a Women’s, Men’s and Pelvic Health Physiotherapist or Nurse Continence Specialist. Doing this in sunlight works faster than it does with PBM.
The Workout You Won’t Want to Miss
Another thing to consider is pelvic floor training with sex. Two musts for a powerful orgasm; a strong, healthy pelvic floor is key and getting the right stimulation along the entire length of the clitoris. Why?
This part of a women releases large electric currents that can help change the fiber type of the pelvic floor muscles.
Women automatically think about the small external portion on top of the vault which is known as the glans—a pleasure zone of nearly 8,000 nerves. That small area loaded with nerves also has the power to spread that oh-so-good feeling to over 15,000 other nerves throughout the pelvis that innervate the muscles of the pelvic floor. The more we can engage those nerve the stronger those muscles get. Let’s just think about the implications of this reality for a moment.
The glans is simply the external portion of the clitoris, but many people don’t know the clitoris extends internally and then splits similarly to a wishbone around the vaginal canal. This means the more of the clitoris we engage the more the muscles of the pelvic floor can become hypertrophied.
If you do not want to do this with your partner consider using medically adapted vibrator for muscle training when you’re alone. Use sunlight or PBM when you do this as outlined above.
Pelvic floor health isn’t all fun and games. Many vibrators were created from a formal medical device. The device above came from a pelvic EMG for nerve damage during birth trauma. These nerve injuries were some of the most difficult I had to deal with as a peripheral nerve neurosurgeon. We had some custom devices we used to help with these injuries but several entrepenurial women came up with the idea to make something they could use at home. This is one example but these days there are a myriad of choices to use to help this problem. It is an example of an intimate health product available that combines pelvic floor toning with training of the muscles, while giving you a workout you’ll look forward to.
The pelvic floor is a group of muscles that surround the vagina and support other structures in the pelvis. Strong pelvic floor muscles provide improved intimacy, sensation and stronger orgasm, along with better bladder control. So yes, orgasms and pelvic floor health are linked ladies by your fiber type, and muscle fiber type is traiable. Both of them can be optimized when you know how to train these muscles.
A general consensus exists among scientists who actually work in this area regarding human skeletal muscle fiber type changes with exercise:
All fiber types change with training, and it happens quickly.
Most sedentary (sexercise) people have ~20-40% of their fibers at hybrids. Active people are usually in the 10-20% range. Very highly trained athletes may have little to no hybrids. So guess what, the amount of sexercise you get matters to your pelvic floor!
Typically hybrids convert to pure types (i.e., MHC IIa/IIx convert to MHC IIa, and MHC I/IIa convert to MHC I or MHC IIa – depending on training style) when any type of training occurs, particularly the MHC IIa/IIx fibers. The reverse happens with disuse = atrophy = incontinence = lack of strong orgasm.
Extremely plasticity exists (i.e., it’s easy to change) between all fiber types, though pure MHC I appear more rigid (but they still do change).
The amount of change is controlled by exposure time and intensity; training more often = more change.
The scientific evidence indicates females have more slow-twitch fibers than men (cite 1 below), and single fiber contractile force and velocity adaptations vary between men and women in a fiber type-dependent and MHC-specific manner (cite 2 below). This all seemingly indicates a need for development of fiber type and gender-specific training programs. This is why I wrote the blog for my tribe of ladies.
SUMMARY
Muscle stimulation provides the “mind muscle connection”, as Intensity automatically strengthens your pelvic floor muscles, it teaches you how an effective, properly performed Kegel exercise should feel—allowing you to learn proper technique. It is no different than lifting in the gym. If your technique is off you will not get the desired muscle strength. With added inflation, Intensity’s vibration activates more nerves, meaning your body is learning to experience more sensation and muscle strength with every training session.
If you find yourself delaying toileting too long, try to make a conscious effort not to. A normal voiding schedule is every two to four hours.
They call it a restroom for reason!
Nature programs in us builds endless optimism in the face of repeated failures. Do not let incontinence or diminished orgasm stop you. In this way Mother Nature forces us to move to act to learn about our world and our body. You have to “open up” to the world and learn optimism to get regeneration. In Nature, you always collect failures on your way to success.
Consider photography in Nature. Not every one is Ansel Adams when they begin. Few learn immediately that the widest, most open, most accepting aperture, the one providing the narrowest, most demanding depth of field is what you need to take a great picture. The same idea cab used to train your pelvic floor. The mechanics of image-making as it related to a women’s pelvic muscles is not an analogy one often finds but it works. For example, using vibration and light simultaneously can be optimized as you can do with a camera. Stopping down the fixed 35mm lens’s diaphragm- which is elegantly composed of nine leaf-shutter blades-to a tight focal length of f/16 would be the equivalent of executing a Kegel pelvic floor exercise. It tightens while gives the most depth of sensation that a muscle needs to train.
CITES
Norman B, Esbjornsson M, Rundqvist H, Osterlund T, von Walden F, Tesch PA. Strength, power, fiber types, and mRNA expression in trained men and women with different ACTN3 R577X genotypes. J Appl Physiol (1985). 2009;106(3):959-65.
Miller MS, Callahan DM, Tourville TW et al. Moderate-Intensity Resistance Exercise Alters Skeletal Muscle Molecular and Cellular Structure and Function in Inactive, Older Adults with Knee Osteoarthritis. J Appl Physiol (1985). 2017:jap 00830 2016.
Williamson DL, Gallagher PM, Carroll CC, Raue U, Trappe SW. Reduction in hybrid single muscle fiber proportions with resistance training in humans. J Appl Physiol (1985). 2001;91(5):1955-61.
Guth L, Yellin H. The dynamic nature of the so-called “fiber types” of nammalian skeletal muscle. Exp Neurol. 1971;31(2):227-300.
Health and wealth are linked in ways most cannot comprehend. What good is wealth if you have no health in which to use it? This simple idea tells you time is your most valuable asset.
What good was Steve Jobs or Paul Allen’s billions when both died of cancers in the mid 50’s?
We can use our BTC wealth to transform medicine by sponsoring researchers who study mitochondrial physiology in lab experiments that are done under sunlight versus laboratory light. Might that small change lead to an end of disease epidemics?
When we entertain our fantasies long enough we often find threads of Nature’s truths buried in them. The simplest things are the most profound.
Destiny can be changed but it requires the energy of sacrifice. Do you trust yourself right now to decide properly what it is that you ought to do?
Whatever one puts out into the Universe will come back to them. What will your payoff be?
Life requires our participation to happen. It does not happen by itself. If not now, when? If not you, who?
One must accept something in order to change it. Why do you accept less than you deserve?
Wherever you go, there you are. It is we who must change and not the people, places or things. All we are given is ourselves. That is the only thing we have control over. You are enough to make the change you need.
If there is something wrong in one’s life, there is something wrong in their environment. Will you learn to use new wealth to change what ails you?
We mirror what surrounds us, and what surrounds us mirrors us. You cannot get well in the same environment you got sick in.
Focus on the task. One cannot think of two things at the same time. Will you cling to what you know now, or sacrifice it for something different?
If one believes something to be true, then sometime in their life they will be called upon to demonstrate that truth. When will you act when fate knocks on your door?
One cannot be in the here and now if they are looking backward to examine what was or forward to worry about the future. Old thoughts, old patterns of behavior, and old dreams prevent us from having new ones. Think about a sats life, not a fiat one.
History repeats itself until we learn the lessons that we need to change our path. No matter how many bad decisions where made, there is still time to change the road you’re on.
All rewards require initial toil. Toil is the toll energy requires for proper change conservation. Nothing worthwhile comes easy in life. Are you ready?
One gets back from something whatever they put into it. The true value of something is a direct result of the energy and intent that is put into it. Every personal contribution is also a contribution to the whole. This is axiomatic of quantum mechanics. Lesser contributions have no impact on the whole, nor do they work to diminish it. If you do not get the desired result, do more.
The smallest or seemingly least important of things must be done because everything in the Universe is connected. Each step leads to the next step, and so forth and so on. Someone must do the initial work to get a job done. Neither the first step nor the last are of greater significance. They are both needed to accomplish the task. Past, present, and future are all connected. We can shrink time when we are plugged into the correct things in life.
The news from Miami is great. Change is here. Jack Mallers onboarded a country and Jack Dorsey met with me and my tribe members in Miami for a two hour POW WOW. I will discuss the details of this with the rest of my tribe during our June Q & A.
El Salvador President Nayib Bukele plans to introduce legislation that will make it the world’s first sovereign nation to adopt bitcoin as legal tender. This is a huge win for El Salvador but it may have just created the best solution for Black Swan mitochondriacs looking to get closer to the sun to improve their health. It also might have unlocked massive value for many because President Bukele also said there will be no long term capital gains on BTC in his country either. Anyone who owns BTC might have been given a huge gift today if they understand how to play it.
Bukele said the country is partnering with digital payment company, Strike, to build modern financial infrastructure using bitcoin technology. I told you earlier in this series everyone needs to use the Strike App for payment rails and now you see why that advice was prescient. You’ll need it when you understand the US tax law that says anyone can transfer 200 dollars per day tax free with another countries legal tender. This is what a Black Swan does……..find a crack where the light can enter.
Bukele’s New Ideas party has control over the country’s Legislative Assembly, so passage of the bill is very likely. This El Salvador headline was embedded in the 686,604th block of Bitcoin blockchain and shall remain there until the end of time.
BTC has a market cap of $680 billion dollars. If 1% of it is invested in El Salvador, that would increase their GDP by 25%. It also adds 10 million users to the BTC network and that incluses 6 billion dollars in remittences to be on chain transactions improving the BTC network. Every BTC miner in the world has to be happy because it means more transactions and more security. A politician from Paraguay (@carlitosrejala) has posted a laser eyes photo and promised a bitcoin announcement this week. Just as we saw MicroStrategy start the domino effect for public companies, El Salvador will likely be a catalyst for other countries.
My 2 hour meeting with Jack Dorsey also revealed his plans around payment rails and global change and his plan to force Twitter to a 100% decentralized social media platform under the plan Blue Sky. He told me it should be done in 12-18 months. We met post sunset under red light without shoes on. For those of you who do not know Mr. Dorsey has followed my biologic teaching for ten years and recently relocated south to help solve some issues he was having. If you look at my Tweets during the Miami event you’ll see I was tweeting at him about his tan and lack of EMF use. He told us that he forgot his blue blockers at his house before he came to Miami. He also mentioned that as soon as he stepped off the plane in Miami he knew he would not feel well in this 5G mecca. He is quite bullish on what BTC means to regular people in the world and asked me to continue to onboard people into the BTC system before the bankers get in. He also told us how his failures at twitter are fueling his growth as a philanthropist in the next part of his life. It was a great conversation.
I spoke to Jack about an idea I got from ClubHouse to create an oasis for ex-pats using lightning networked nodes. It will use a distributed ledger technology, like blockchain, are peer-to-peer networks that enable multiple members to maintain their own identical copy of a shared ledger. Rather than requiring a central authority to update and communicate records to all participants, DLTs allow their members to securely verify, execute, and record their own transactions without relying on a middleman. In this way, we can move away from all institutions who are not trustworthy. We want a world without censorship.
While there are a wide variety of DLTs on the market, they are all comprised of the same building blocks: a public or private / permissioned / permissionless distributed ledger, a consensus algorithm (to ensure all copies of the ledger are identical), and a framework for incentivizing and rewarding network participation.
Distributed ledgers are categorized as “private” or “public” and “permissioned” or “permissionless” — they can be any combination of any of the two. To achieve full decentralization, I believe distributed ledgers must public permissionless networks. Mr. Dorsey seemed to like this idea and invited me to his house to discuss it and invest in it with me and why I want to use it for decentralized medical practice.
Public / Permissionless DLT is a type of network is the most decentralized. Applications can be deployed in production or removed, without having to notify anyone, reveal their identity, or meet any application criteria requirements. Additionally, the nodes which constitute the network can freely and anonymously join and contribute, typically in exchange for a network’s native cryptocurrency. In our case, I want that to be 100% BTC. He agrees. He sees no need for any other crypto and he told me this is why Square is a BTC only platform. It also speaks to how he values self sovereignty and a lack of censorship.
Why was I happy to see Mr. Dorsey smile at this idea? It told me he was someone who sees the world as I do. We have inalienable rights and no one should limit them.
Because central ledgers rely on intermediaries, they are burdened by the costs and inefficiencies of the middleman. DLTs do away with these limitations by avoiding middlemen and intermediaries altogether. Without a central agent, there is no need to pay a central agent. And, without the need for clunky bureaucracy, you can exchange assets directly and immediately. You no longer have to limit the speed of your transaction to the efficiency of expensive bankers, lawyers, or politicians. He gets why I love this idea.
Moreover, you no longer have to trust bankers, lawyers, or politicians with the ledger and your assets. DLTs are trustless systems, meaning that no participant needs to trust any other participant to guarantee a valid ledger.
Traditional ledgers may provide fast and simple record-keeping, but they are vulnerable to corruption and hacking. Because only one central entity controls the ledger, a corrupt central agent can tamper with the records without the consent or knowledge of the affected members. Moreover, because there is only one copy of the ledger, hackers have a clear, single target for their attacks. Without visibility into whether tampering has occurred, we must simply trust that the central third-party is neither corrupt nor compromised when we use a centralized ledger.
Distributed ledgers, however, are inherently resistant to tampering. While a malicious agent could compromise a central system by altering the single ledger, they would need to alter at least a plurality of ledgers to have an impact on a distributed system.
Though DLTs are not tamper-proof, they are tamper-apparent. That is, if tampering does occur, the network’s transparency ensures that all members of the network will be aware of the change. Once it is apparent all we would have to do is turn off the node that is the bad actor and that is all it takes to secure the network. This type of system could be used by a group of “Black Swans” who want to create their own 51st state virtually anywhere in the world. It offers self government by the people who participate with their own node in this network. This is the type of change I have wanted to see in the world to force change in many paradigms. I’m here to tell you Mr. Dorsey sees the new world in the exact same way and wants to invest in this idea.
Our centralized world has failed us. Mr Dorsey said this to all of us about Twitter’s censroship. He knows it must change and wants to be part of this change. The failure around Twitter has made him see where he needs to go.
SUMMARY
Failure is the best teacher in Nature.
Mistakes are opportunities for error correction. Error correction is a sign of intelligence rising. Decide to embrace today’s fiat chaos.
A funny thing happens when you embrace the suck. A funny thing happens when you embrace your strengths or limitations – you become better able to embrace its opposite. This means you increasingly step into your true self and start to understand that failure is the best teacher.
See it as a gift: When you’re willing to accept your limitations, everyone around you breathes a bit easier. This is because when you accept your shortcomings, you create an environment of love and acceptance that helps helps everyone around you heal, themselves.
Karma is a lifestyle that promotes positive thinking and actions.
Karma is not meant to be a punishment. It is present for the sake of education. How else is someone to learn how to be a good person if they are never taught that harmful action is wrong? A person only suffers if they have created the conditions for suffering. You control your own destiny with the decisions you make and act upon.
The El Salvador news will likely bring up the topic of ending the dollar as a world global asset soon. This is a needed step before we get the BTC Standard. Why? The use of a national currency, such as the U.S. dollar, as global reserve currency always leads to tension between its national and global monetary policy. Every President since 1945 has faced this issue in one way or another. This is reflected in fundamental imbalances in the balance of payments, specifically the current account, as some goals require an outflow of dollars from the United States, while others require an overall inflow. This change always leads to massive trade imbalances. Many people do not realize that this is one reason why I believe the US Treasury wants to end the dollars reign as the global reserve currency. It now is a net negative to US economic growth at the end of this debt cycle.
The problems with the role of the U.S. dollar as the reserve currency under the Bretton Woods system first manifested in 1959. This occurred due to money flowing out of the country through the Marshall Plan, U.S. military budget and Americans buying foreign goods, the number of U.S. dollars in circulation exceeded the amount of gold that was backing them in 1959.
By the autumn of 1960, an ounce of gold could be exchanged for $40 in the London market even though the official rate in the United States was $35. This price difference was due to price controls on gold in the US which was fixed by the US government in 1933 following the implementation of Executive Order 6102. In USD terms, the price of gold had not changed in 27 years, but this did not allow true price discovery by the free market. This price was fixed following the enactment of E.O. 6102, where the US government purchased gold from US citizens under threat of fines and/or jail time at a rate of $20.67/oz, then quickly revalued the gold to $35/oz.
In order to maintain the Bretton Woods system, the US had to run a balance of paymentscurrent accountdeficit to provide liquidity for the conversion of gold into U.S. dollars. With more US dollars in the system than were backed with gold under the Bretton Woods agreement, the US dollar was overvalued. The gold reserves of the United States were reduced as foreign governments converted US dollars to gold and took it offshore. This was due to price arbitrage.
This implies in a BTC Standard world no one will want to be considered the global reserve currency. It always leads to unintended consequences for the nation that has it. BTC solves this problem because it has no leader is 100% decentralized.
As with all price controls, this caused supply and demand imbalances and an arbitrage opportunity which rapidly depleted the United States gold reserves in the 1960s. This is when China and Europe began to buy gold at the US Treasury. This led to less gold in the country and caused the US Dollar to become even more overvalued relative to the US gold reserves, leading to a self-propagating cycle. Furthermore, the US had to run a balance of payments current account surplus to maintain confidence in the US dollar at this time. Ultimately, this is why in August 1971 the gold standard was ended by Nixon.
The United States was faced with a dilemma because it is not possible to run a balance of payments current account deficit and surplus at the same time. Nixon was prodded by Kissinger and his friends at the World economic forum to acknowledged the demise of the Bretton Woods system and let the US dollar float because of the superiority of the US miltitary to prop up the Federal Reserve. Nixon announced that the dollar could no longer be exchanged for gold. This solved the gold reserve problem but opened the door to public thievery of the politician and industrial military complex by allowing the Fed to expand the money supply and effectively steal money from the taxpayers of the US the last 50 years by debasing the currency.
In August of 1971 Nixon announced it as a temporary measure, it was to remain in effect for the last 50 years because stealing became a way of life for the Congress and Executive branch. When the “gold window” was closed for good a new problem began for America. Central bank inflation was born and is now a legalized form of counterfeiting and counterfeiting inside the beltway. This has become criminalized inflation of all US taxpayers.
Owning BTC solves this problem for the US taxpayer.
It seems Jack Mallers, Dorsey and Kruse all understand this and are on the same team now.
Post Miami, I remain wildly bullish on how BTC can change our world.
Russell van Gelder, M.D., Ph.D., a professor of ophthalmology at the University of Washington, studied the circadian rhythms of genetically tweaked mice that were missing rod and cone cells and melanopsin. As expected, the circadian rhythms of these mice continued cycling but could no longer adapt to changes in light exposure. Surprisingly, though, the activity patterns of their retina’s were still responsive to light changes, suggesting that there was another light photoreceptor in play in the eye and skin. That pigment was neuropsin.
This opsin, like all opsins, work with the Vitamin A cycle in the body. Most people struggle to convert dietary carotenoids into the active form of Vitamin A needed for photo-reception. It turns out that blue light toxicity on the eyes or skin ruins the conversion of dietary carotenoids to retinol and this causes circadian phase delays that underpin mitochondrial diseases.
This opsin discovery is when I began to realize all I was taught about the sunlight in medical might be a fallacy. The current paradigm in ophthalmology says that UV light is really bad for the eye and skin. Well, if that was true why would Mother Nature have put a UVA opsin in the cornea and in the skin.
Yep, neuropsin has been found in the eyes, skin, and subcutaneous fat now mimicking the exact spots where melanopsin is found. Could this be why light at night leads to myopia and fat as I laid out in my Vermont 2017 video on youtube? It does appear that the sensations your eyes get from light gives us the reality we experience here on Earth.
LETS JUMP DEEPER.
The retina is the only tissue known to ignore the master clock based in the SCN, but it does keep itself on a schedule, based upon all the data we have. That made me ask the question, how does this occur?
I looked at articles where opsin were removed from animals (see above). It turned out the retinas of the mice without neuropsin lost their ability to adapt to new patterns of light and darkness. I found out that neuropsin and melatonin function must be coupled because melatonin is the hormone of darkness that is regenerated by daytime later morning UV light (9-11AM). Was neuropsin key in this recycling of melatonin? Does neuropsin also work with UV light in some way during the day?
The scientists working with these mice began by repeating their experiments with different wavelengths of light, the they found that neuropsin responds to UV-A and violet light up to 400 nm. This implied that the retina uses separate light signals based upon frequency to set its own clock and that of the body’s master clock in the SCN. The central retinal pathways controlled by melanopsin are exquisitely sensitive to light in 435nm-465nm light which is based in the blue/green part of the spectrum. 400-430 nm light is present in early AM sunlight, before UVA shows up, and it becomes very prominent at dusk when the sun slowly sets. These frequencies of light are ideally absorbed by melanopsin over several hours at dusk. Melanopsin can be thought of as an opsin that pays attention to light as it dims. Regarding neuropsin, we still don’t know precisely what kind of signals, either photonic, chemical or electrical, that neuropsin uses to set the retina’s clock. My current bet it will be found to be photoelectric because of another clue the eye has given us. Neuropsin is found in the cornea and the skin and this makes it very unique. Why would we have a UV-A light sensor for bright mid-day light frequencies in a transparent cornea? Since neuropsin works via UV-A light this is a “tell” that our modern beliefs that the cornea and lens block UV light is a pure fallacy. It also tells us that non UV-B sunlight is important to melatonin recycling.
How did we find out neuropsin was in the cornea? Researchers used a specialized “locator gene,” called a reporter gene, to figure out where neuropsin does its work. They found that, like melanopsin, it is located in neural cells that connect the retina to the brain via the central retinal pathways. From there though, we do not know precisely yet today where these particular cells go within the human brain. Using this technique they did mysteriously confirm it is present it in the cornea. This shocked many, including the eye doctors. The cornea was not thought to contain any UV pigments by ophthalmologists, since its job is to let light through to the rest of the eye. We now know this data needs updating.
MY BELIEFS ABOUT NEUROPSIN AND IT LINK TO UV-A LIGHT
I currently believe neuropsin was selected for by the KT event in eutherian mammals that made it through the last extinction event. During this time it is believed that photosynthesis was disrupted for several decades to 1000 years. This would have lowered the quantum yield of sunlight on the entire planet. A lowered quantum yield of sun light would have sharply lowered UVB light more than UVA light.
Watching the light at the sunrise at 15% angle gets best results for health. This angle is when the red light predominates. As the angle gets over 15% UVA shows up. Over 30% is when UVB light has arrived on most places on Earth.
Mammals that survived would have needed some way to get environmental signals to their pituitary gland to drive the thyroid hormone cycle needed to drive seasonal changes and to control reproduction. Without these two factors, no mammals would have survived very long, in a low quantum yield environment. In today’s world, we now see the same similarities in our environment but for different reasons. As a result, in humans, thyroid diseases and fertility changes are now at pandemic levels. I believe that UV-A light is critical in driving thyroid cycling in all modern mammals including humans. When we see massive spikes in hypothyroidism, it is a sign that there is a global lowering of the quantum yield of sunlight for some reason. 65 million years ago it was debris from an asteroid that cause blockade of specific frequencies of light. Today, it is non native EMF in the ionosphere that are destructively interfering with sunlight that falls to the Earth surface. This explains why we have a global Vitamin D3 pandemic and why we see massive spikes in hypothyroidism and infertility. Free T3 is needed for fertility (leptin) and for nerve function. Low free T3 levels also are associated with chronic pain and severe alterations in cardiac function. Free T3 levels have been studied in post heart surgery patients and been found to be an very good reliable outcome measure. Free T3 tends to trend with melatonin levels because both need UV light exposure to recycle themselves in mammals. Low free T3 levels is a sign of low UV light exposure.
Since eutherian mammals made it past this event horizon it stands to reason that this gene should be highly conserved in all mammals that survived. So what does the data say about my idea?
Within placental mammals, neuropsin is extraordinarily conserved, with percent identity relative to human protein 96% averaged over 31 species; exceeding the 95% percentile of all coding genes proteome wide! That conservation drops considerably at marsupials and monotremes (86%), is less striking at tetrapods (78%), and not especially remarkable at teleost fish (68%). This pattern suggests neuropsin acquired significant new adaptive functionality on the placental mammal stem, leading to marked resilience to fixation of any further variation for the last 65 million years. That is why I believe as I do today. My beliefs are always subject to new data.
Does this explain why the modern world faces a pandemic of hypothyroid disease?
It might. Why? How does this link to thyroid function? Most people in medicine today know about thyroid function but few can explain why hypothyroidism is now at pandemic levels. I think a global lowered quantum yield of sunlight on Earth maybe the reason. This sounds hard to fathom, because few really understand how the thyroid is controlled by light. In 2010, I came across a study that gave me some insight to build upon this idea that I wrote about in Cold Thermogenesis 4 and Cold Thermogenesis 6. Thyroid function, cold, and UV-A light exposure had to be linked in some way that biochemistry and medicine have not yet fully appreciated. The linkage seems to go all the way back to the last time the Earth faced a lowered quantum yield. The KT event was the last time Earth faced a “serious brown out from the sun”. Neuropsin evolution was likely how life back then dealt with the last brown out to survive the event. I believe neuropsin isoforms were re engineered in the early eutherian mammals and therapy dinosaurs to absorb in the blue range to overcome the loss of sun light. This helped them live in a low quantum yield world and also allowed them to uncouple their inner mitochondrial membranes to make more heat. This radically changed mitochondrial haplotypes in eutherian mammals. The UV-A neuropsin has re-evolved in mammals as the sun’s power was restored. The link of blue light neuropsin’s in bird and nocturnal mammals links to melatonin regeneration explains why life could survive in a world without full spectrum sunlight. After the asteroid impact UVB light would have been non existent on Earth because of the particulate matter in the atmosphere. UV-A light would have been present but rare. This is why I knew to look at the skin and eye surface for a possible link for a light sensor for blue light. I looked at the other animals that made it through the KT event beside eutherian mammals. They were the therapod dinosaurs. Their modern correlates are birds. Quails happen to be birds.
The 2010 study I mentioned earlier was about the quail brain. It mapped the bird version of neuropsin (NEUR1) to the paraventricular organ, a region of the diencephalon of nonmammalian vertebrates containing aminergic neuronal cell bodies (biogenic amine correlates in mammals) beneath the epithelial membrane lining the third ventricle. The Paraventricular region is where the PVN is located and controls the sympathetic nervous system and it very sensitive to the UV spectrum of light from the retina. The PVN is critical in the stress response and ROS signal from mitochondria from many different environmental signals. This peaked my interest because of what I imagined occurred globally 65 million years ago, to the quantum yield of sunlight, off the coast of Mexico. The modern vertebrate forebrain’s diencephalon also contains the thalamus, hypothalamus and posterior pituitary. This linked many areas of the mammal brain to vital functions.
WHERE DID NEUROPSIN COME FROM? A change in light.
The specific idea laid out in this paper was that incident UV-A and violet light would be sparsely present, but would be clearly able to be detected by the bird version of NEUR1 opsin in paraventricular neurons. This would allow signaling via cerebrospinal fluid to the pars tuberalis of the pituitary gland, inducing there thyroid-stimulating hormone was present. This, in turn, would induce the thyroid deiodinase DIO2 in tanycytes lining the third ventricle to affect fecundity and seasonal adaptations. The 3rd ventricle is filled with CSF, which is 99.8% water. Light changes the hydrogen bonding network in the water. Light and water are critical in forming life’s battery over the 4.5 billion year history on Earth. This interaction would lead to a photo-electric signal in the hydrogen bonding network in CSF that transforms light energy into the lattice of protons produced during a daylight long signal.
This signal induced T3 in the mediobasal hypothalamus, and ultimately could have induce gonadotropin-releasing hormone to the testis and ovaries to control seasonal reproduction. Light and metabolism have always been linked to fecundity in birds and mammals. These are critically important factors, as I laid out in the last chapter of my book, The Epi-paleo Rx. In this paper, they mentioned something rather startling to me about light frequencies and the bird opsin. The peak adsorption was observed to be at 420 nm (blue) in this opsin and it was not readily transferred to orthologs in other species. They found this out by studying genomic alignment and tuning residue formulas. This meant birds faced something rather unusual in their evolutionary past, and it changed their genome in a specific way tied to light. Their opsin responded to a predominance of blue light in the environment? Why would birds have an opsin that responded to blue and not UV light? Moreover, why would nocturnal mammals also have blue light neuropsin’s and why would humans have an opsin that responded to UV-A light?
The KT event fits this scenario quite well because of the brown out the two surviving animals were birds and small nocturnal mammals. I do not believe it is a coincidence that 420 nm is right below melanopsin’s ideal optical range in today’s modern versions of mammals. This made a lot of quantum sense to me considering what an asteroid would have done to the sun’s power and how it would have shuttered certain frequencies between the UV and blue band during daytime hours.
A commentary piece assigned to this article linked the the paraventricular organ to the hypothalamus in modern animals. I immediately thought about the paraventricular nucleus (PVN) in humans. I went digging and found that even though no exact mammalian anatomical counterpart exists completely, the Allen Brain Atlas shows mouse expression of NEUR1 there (blue range). Things began to become more clear. This had to be how light and water helped birds and mammals survive the KT event. They survived because they has strong regeneration programs despite the fact UV light was nearly absent after this event. These animals were able to navigate a low quantum yield event, by innovating an opsin in the skin and eye that responded best to a world that had buried the sun because of a bollide. This version of opsin allowed them sustain higher heteroplasmy percentages because they used the relative darkness of their environment to control regeneration. Melatonin was more important to these animals 65 million years ago than leptin was due to the decreased amount of daytime UV light. Plants are also capable of using blue green light in their photosynthetic centers too to sustain the food webs to allow for a recovery.
The hormone that controls dark = melatonin. When quantum yields are low from sunlight for any reason, sunlight would be like AM sunlight is today up to an angle of 30%, darkness would be more plentiful. There would have been equal parts of blue, green, and red with some critical UV-A light after such an event. The particulate matter would have lowered the amount of UV light considerably in the UV-B range. This environmental change of light might have optimized neuropsin protein to UV-A light.
This is how I believe neuropsin and melatonin made their alliance from an evolutionary perspective 65 million years ago in birds and eutherian mammals. This all of course, assumes that the photoperiodic reproduction hormomal control had to be directed by the light and dark mechanism under melatonin’s control. It should be no surprise that even today, melatonin levels control mitochondrial DNA heteroplasmy percentage. Leptin does not control this process. This tells me on evolutionary time scales varying light on Earth had to be intimately involved with this biologic change. This was a big clue for me why we are seeing the diseases we do today when we now live indoors under man made blue light. This gives melatonin the master control switch that deals with the percentage of heteroplasmy and mito-nuclear co-aptation that Doug Wallace has laid out for modern biology.
This melatonin/neuropsin mechanism is retained from the ancestral situation in all animals that survived the KT event. Even today, the paraventricular organ is known from teleost fish and frog as well as birds. Photoentrainment of daily circadian activity rhythms should be expected to be quite distinct in terms of opsin use from photoreceptor control of seasonal reproduction. This idea fits precisely with what we now know about the human NEUR1 transcripts most commonly recovered from testis and ovary. Want some proof for this speculation I am bring forth to you here? Google neuropsin transcript DB097202. It has a massive phylogenetic range back to amphioxus and sea urchins, past which, unfortunately nothing is known today.
SUMMARY
Knowing is not enough; we must apply the knowledge. Willing is not enough; we must do the right thing around light in the decentralized web Nature gives us on Earth or it will sculpt us in ways we not be ready for.
Nature programs in us builds endless optimism in the face of repeated failures. In this way she forces us to move to act to learn about our world. You have to open up to the world and learn optimism. In Nature, you always collect failures on your way to success.
Nighttime rumination about the Federal Reserve: They say our experiences, stories, and lessons in life are not for us but for others. What might I do to serve others and not just myself? I don’t believe we are here to serve or engage ourselves but to serve others and engage them with the purpose of accomplishing a higher purpose greater than ourselves. It clear our leaders feel differently because of the way they support Fed monetary policy.
To execute quantitative easing, central banks increase the supply of money by buying government bonds and other securities. Increasing the supply of money lowers interest rates. When interest rates are lower, banks can lend with easier terms.
In theory QE, in turn, spurs economic growth. Today the debt to GDP ratio is so high that growth is now impossible.
A high debt-to-GDP ratio is undesirable for a country, as a higher ratio indicates a higher risk of default. In a study conducted by the World Bank, a ratio that exceeds 77% for an extended period of time may result in an adverse impact on economic growth.
Government Debt to GDP in the United States is now 120 percent in 2021. At curent QE rates the national debt will approach $89 trillion by 2029 according to USDebtClock.org. This would put the country’s debt-to-GDP ratio at 277%. This is unsustainable.
Above 90 percent of GDP, median growth plummets further, and average growth actually turned negative. The maturity of the debt also plays a factor, with nations heavily reliant on short-term borrowings most vulnerable to sudden crises. The USA is now way over the 90% threshold. This is why foreign governments stopped by US T Bills at US Treasury auctions in 2015.
CBO projects a federal budget deficit of $2.3 trillion in 2021, nearly $900 billion less than the shortfall recorded in 2020. At 10.3 percent of gross domestic product (GDP), the deficit in 2021 would be the second largest since 1945, exceeded only by the 14.9 percent shortfall recorded last year. Those deficits, which were already projected to be large by historical standards before the onset of the 2020–2021 coronavirus pandemic, have widened significantly as a result of the economic disruption caused by the lockdowns by government decree during the pandemic and the enactment of legislation in response.
Quantitative easing stimulates the economy in three other ways.
QE Keeps Bond Yields Low
The federal government auctions off large quantities of Treasuries to pay for expansionary fiscal policy. It increases demand as the Fed buys Treasuries, keeping Treasury yields low. (There’s an inverse relationship between yields and prices with bonds.)
Treasuries are the basis for all long-term interest rates. Quantitative easing through buying Treasuries therefore also keeps auto, furniture, and other consumer debt rates affordable. The same is true for long-term, fixed-interest debt. It supports the housing market when mortgage rates are kept low, and low rates on corporate bonds make it affordable for businesses to expand.
QE Attracts Foreign Investment and Increases Exports
Increasing the money supply also keeps the value of the country’s currency low. U.S. stocks are more attractive to foreign investors when the dollar is weaker, because they can get more for their money. A cheaper dollar also makes exports less expensive abroad.
QE Could Lead to Inflation
The only downside is that QE increases the Fed’s holdings of Treasuries and other securities. For example, the Fed’s balance sheet held less than $1 trillion before the 2008 financial crisis. That number had increased to almost $4.5 trillion by July 2014. Today in 2021, it is now 30 Trillion dollars.
The more dollars the Fed creates, the less valuable existing dollars are. This lowers the value of all dollars over time, which then buys less. The result is inflation.
Why did the Federal Reserve go from emergency lending in 2008 to quantitative easing?
The Fed launched four rounds of QE to fight the financial crisis in 2008. They lasted from December 2008 to October 2014. The Fed resorted to QE because its other expansionary monetary policy tools had reached their limits. The fed funds rate and the discount rate were zero. The Fed even began paying interest to banks for their reserve requirements. Quantitative easing became the central bank’s primary tool to stop the crisis.
First – this blog is not tax advice. Please consult with a tax lawyer or CPA before doing your taxes, and hey, it goes without saying, but always pay your taxes.
One USD dollar invested in Bitcoin in 2010 is now worth 900,000 dollars. Great news, but how much in taxes do you owe if you sell it?
The news is good if you did not sell and still own it.
Starting in the 2020 tax season, on Schedule 1, every taxpayer has to answer at any time during the year whether you receive, sell, send, exchange, or otherwise acquire any financial interest in any virtual currency as the video above said.
This is an extremely broad question and will require you to check “yes” even if you are just holding crypto in an exchange or wallet. In 2020, the IRS clearly sees noncompliance on virtual currency transactions as a threat to the tax system.
If you mark “yes”, first & foremost, it would signal the IRS to check various forms and schedules of the return for cryptocurrency gains and losses. However, everyone who marks “yes” may not have a reportable taxable event. For example, during 2019, if you just held bitcoin and did not sell, you would not have any taxable amount to report. In these cases, the IRS will use the cryptocurrency question as a way to gather data about US crypto holders and keep an eye on future years for taxable events. HYPERLINK
The IRS sent three different types of notices in the initial phase in 2019: I know because I got one from them via the Bitstamp exchange.
Letter 6174– this wass a soft notice informing the taxpayer that there is a likelihood that they did not report their virtual currency transactions. The notice asked them to re-check their return and, if necessary, file an amended return to correct the misreporting. The taxpayer is not required to respond to the notice and the IRS intends not to follow up on these notices. In short, this is information only to the taxpayer and education on how they comply.
Letter 6174-A– this was a “not so soft notice” from the IRS. As in Letter 6174, this letter tells the taxpayer that there is potential misreporting of virtual currency transactions. However, this notices stated that the IRS may follow-up with future enforcement action. Again, no response was required if the taxpayer believes that they are in compliance. Taxpayers who received this notice should have been aware that they have been put on “notice” that they have been identified as a noncompliant taxpayer for potential future IRS enforcement (audit)
The last notice required a response – Letter 6173. This notice requested a response from the taxpayer about the alleged noncompliance. The letter provided instructions on responding to the IRS. The IRS intends to follow up on these responses to determine if the taxpayer is in compliance.
The IRS started sending a small number of these notices in June, 2019. Mass mailing of these letters will occur during the week of July 22, 2019, and continue through August. Taxpayers receiving this notice will have a special hotline and address at the IRS for any contacts and responses
Bitcoin however, enjoys a favorable tax treatment from the IRS. This is bullish considering its run in 2019. They key is understanding your tax basis and why it should be held for investing purposes but also for its tax treatment.
Capital gains tax in crypto is especially bad because it is extremely expensive to rotate positions in a bull market. Your next investment needs to outperform your current hold by 30-40% to be in the money net of tax. This is why I tell everyone never sell once you buy.
Most talk about why you should never sell BTC, but if you do sell you need to know what your tax basis is. As with all financial advice, check with your tax expert before taking any advice from anyone. So what does the IRS say about BTC/GBTC tax basis?
According to the IRS’ official guidance on crypto taxation, crypto is taxed as “property,” which is just a fancy way to say it’s taxed like a stock.
Thank the Bitcoin God!
Now let’s go back in history to 2010 and see what BTC founder had to say about this aspect of BTC: “Bitcoins have no dividend or potential future dividend, therefore not like a stock. More like a collectible or commodity.”
The US government decided to handle BTC differently. Why?
If you buy bitcoin and hold it for more than a year, you pay long-term capital gains when you sell. For US federal taxes, that means you pay a 15% tax on any gains, unless you make a lot of money (more than $479,000 (for married couples) or $425,800 (for individuals)), in which case you pay 20%. That compares favorably with almost every other alternative investment sold on Wall Street exchanges.
I believe there were two main reasons the government did this. The first one is obvious.
1. Taxing it like a stock makes it very unfavorable to be used as a currency to compete with the US Dollar. They do not want any competition for the dollar because of how they use the dollar to punish countries politically and exert pressure.
2. The second reason was to use IRS tax law to uncover who holds cryptocurrency so they could tracked and surveilled for tax purposes into the future.
The government knows tracking crypto transactions is difficult for the IRS because of manpower. They also know that the cell phone is the ideal way to track people who own crypto. This is one reason why using a VPN on your phone/computer is very wise at the beginning of 2021. The IRS is telegraphing they intend to have the NSA spy on us through our phones. Once they find out who admits they have crypto they’ll know who to surveil via technology. This is why everyone who uses cryptocurrency should consider a VPN for their phone.
Eventually, people will think ‘My phone is spying on me’.” Why are they doing this? Under observation, we act less free, which means we effectively are less free. You have to think critically to know what they government will do when the deck is stacked against them in the crypto-world.
For instance: GOLD IS NOT AS BITCOIN FRIENDLY AS BTC when it comes to taxes.
Gold is taxed as a collectible. That means, no matter how long you hold it, the lowest tax you can pay when you sell is 28%. And yes, this is true even if you hold a gold exchange-traded fund like the SPDR Gold Shares (GLD); there’s nothing magical about wrapping physical gold in an ETF that changes its tax treatment.
Currency is taxed at regular income rates. No matter how long you hold a currency investment like the Invesco CurrencyShares Japanese Yen Trust (FXY), you never qualify for long-term capital gains. Instead, you pay your marginal income tax rate on any gains, up to 37% on federal taxes. This one hurts the pocketbook.
Commodity futures–and ETFs that hold commodity futures like the US Oil Fund (USO)–are what’s called Section 1256 contracts for tax purposes. That means two things, neither of which are good for long-term investors:
First, any investment in a Section 1256 contract is “marked to market” at year-end, which means you owe taxes on paper profits at the end of the year even if you don’t sell.
Second, regardless of your holding period, 60% of any gains are considered long-term capital gains, and 40% are considered short-term capital gains. That means the blended tax rate for someone in the highest federal income tax bracket is 26.8%.
The relatively high tax rate is unfortunate, but it’s the mark-to-market feature that kills long-term investors. People really don’t like paying taxes on paper profits, and the inability to defer taxation can have a meaningful impact on long-term returns.
Bitcoin futures, for what it’s worth, are considered Section 1256 contracts, so they fall under this tax classification; direct holding of “physical” bitcoin (or investing in a fund that holds bitcoin) does not.
WHAT ABOUT THE TAX BASIS OF AIRDROPS AND HARD FORKS FOR BTC?
An airdrop, in the cryptocurrency business, is a marketing stunt that involves sending coins or tokens to wallet addresses in order to promote awareness of a new virtual currency. A hard fork is a radical change to the protocol of a blockchain network that makes previously invalid blocks/transactions valid (or vice-versa).
A “hard fork” of a cryptocurrency owned by a taxpayer does not result in gross income for a taxpayer if the taxpayer receives no units of the new cryptocurrency, but taxpayers receiving an “airdrop” of units of a new cryptocurrency after a hard fork have ordinary gross income from the airdrop, the IRS ruled in Rev. Rul. 2019-24, issued in October in 2019. The IRS also updated its Virtual Currency Transactions frequently asked questions on its website to reflect the ruling.
The last thought: the US tax system relies on a voluntary compliance system. This means that the the IRS expects you to report all taxable transactions (whether the IRS knows about those transactions or not)
The IRS is now asking you to self report what crypto transactions on your 1040 return you have made in 2020 because without this information they are flying blind to a degree. They do get some help however. If you receive a Form 1099-K or Form 1099-B from a crypto exchange, without any doubt, the IRS knows that you have reportable crypto currency transactions. … If you receive a Form 1099-B and do not report it, the same principles apply. Likewise, Coinbase, Kraken and other US exchanges do report to the IRS.
This is thanks to the “matching” mechanism embedded in the IRS Information Reporting Program (IRP). During any tax year, if you have more than $20,000 proceeds and 200 transactions in a crypto exchange, you will get a Form 1099-K indicating proceeds for each month. The exchanges are required to create these forms for the users who meet the criteria. A copy of this form is provided to the account holder, and another copy goes to the IRS. If you file a tax return and do not include these amounts, the IRS computer system (Automated Underreporter (AUR)) automatically flags those tax returns for under reporting. This is how you get tax notices like CP2000. If you receive a Form 1099-B and do not report it, the same principles apply.
Over the past few years, the IRS has issued subpoenas to several crypto exchanges ordering them to disclose some user accounts. Many crypto investors got caught in that web after the 2017 drop because many people sold BTC and did not hold it. This created huge IRS interest. Word is this is another reason why IRS decided to treat BTC as a stock to get more tax monies. Anyone who sold it at a loss would want to offset the loss with a gain so the IRS could find out how many Americans were really holding cryptocurrency.
For example, in 2018, Coinbase had to disclose approximately 13,000 user accounts including taxpayer identification number, name, birth date, address, records of account activity, transaction logs and all periodic statements of account or invoices (or the equivalent) pursuant to John Doe summons. On another occasion, the IRS subpoenaed Bitstamp to release more information about a taxpayer who filed an amended return and requested a $15,475 refund. Let’s just say I know that taxpayer and how the IRS tracked the person of interest.
A 2020 point: If you took a crypto loan from an exchange remember the interest is tax deductible but the loan amount can be calculated from the interest paid. This tells the IRS that a balance had to be present on the exchange at some point to make the collateral based loan.
IS DeFi HANDLED DIFFERENTLY?
That was all Bitcoin, what about Defi crypto transactions on Etherium?
There are three big topics in DeFi to cover for taxes – liquidity pools, staking and yield farming, and NFTs.
Very simply, a liquidity pool, or a DEX, is a smart contract where you can exchange one token for another. I have written about them already in the BTC series. Have a look at them.
Trading on a DEX is exactly the same treatment as trading anywhere else. There is one level of complexity which is that Dex’s are 100% token to token trades, as opposed to exchanges where one side of the pair is often a fiat currency.
Liquidity Providing
But, let’s talk about the DeFi part – providing liquidity to a pool. I pick a pair (let’s say the SushiSwap WBTC / WETH) and I deposit 50% value of each asset. For instance, in March that would be around 1 WBTC and 25 WETH. As part of that deposit, I get a token back indicating my ownership percent of the pool. People then trade against that pool, and over time my holding will shift in line with the relative movement of WBTC and WETH. Perhaps in a week my holdings will be with 1.1 WBTC and 24 WETH.
There are a few ways people are treating this for tax purposes. On the one hand, some people treat the initial deposit and token issuance as a trade. That is to say, you’re 100% disposing of the WBTC and WETH, and acquiring a new token with the cost basis of the tokens you disposed of.
For a lot of people, this is a perfectly reasonable treatment, especially if you only recently got into crypto. That’s because you pick up a gain or loss based on that disposition – if you’ve been hodling a month that might be a minor loss. If you’ve been hodling 5 years, you may be creating an enormous tax bill for yourself which would require you to liquidate assets.
To deal with that problem, some tax professionals are recommending you treat this as a containerization – the best analogy is to think of a blind trust. Back in the day, politicians would put their assets into a blind trust when they took office, which is to say they didn’t sell all their stock, but they put it under the care of a professional who would not consult with them on trades. Theoretically, this decreased the chances of the politician making self-enriching policy.
In that case, the transfer to the blind trust was not a taxable event, but every trade that the blind trust executed would be even if you weren’t directing it.
That’s essentially what a liquidity pool is – you deposit some funds, then other people are actually doing the trading on top. So, in a perfect world, you’re not recognizing the transfer into the pool as a taxable event, you’re monitoring the trades and recognizing those on a block by block, day by day, or month by month basis. We build software to automate that, but you can do it yourself by just picking a time once a day to check your underlying asset balance in the liquidity pool, recording that in a spreadsheet, then having a column that tracks the relative deltas of the assets. Turning that into a trade can be simple for a 2 asset pool, perhaps more complex for a pool like Balancer, and you have to follow some rules around multi-asset trades.
In this way, you are essentially only recognizing the change to your holdings, not a full sale of all your deposited crypto. In fact, a similar discussion arises around WBTC and WETH – is the movement from ETH to WETH a sales and acquisition, or a containerization? Some tax professionals are ok with the containerized approach, some aren’t – so, talk to your tax person before you jump into this world!
FOR DeFi TRADING CONSIDER A CORPORATE CRYPTO ACCOUNT
Interestingly, in the eyes of the law, Corporations are afforded similar rights to natural living humans. Corporations have the right to transact, own assets, buy and sell property, and conduct business – as the business deems fit, as a legal person.
Corporations function under what is known as a corporate veil. This is an important distinction that separates the actions of the corporation from the actions of the business owners (shareholders) and it also affords protection to the shareholders from being liable for the corporation’s actions.
A Corporation has many of the same rights as a natural person and more rights than a natural person — under the age of majority (minors are not permitted to enter into legally binding contracts).
Suffice it to say, the legal status given to a corporate entity makes it a very powerful vehicle to conduct business and offers significant tax advantages and asset protection when compared to transacting as a natural person. Your tax professional can help you figure out how to maximized this option for your needs.
Yield Farming & ETH 2.0
What about staking and yield farming for tax purposes?
There are a lot of great articles about how to do taxes on mining revenue, and for the most part you can follow that guidance for staking and yield farming as well. Let’s take the above example – I want to deposit my SLP token and earn some SUSHI yield on that. Because you retain full control over those staked assets, and can remove them any time, you can really think of this as a bank account that’s earning interest. There is then the same debate about the staking rewards as there already exists about mining – namely, do you treat it as income immediately when it hits your wallet, or do you treat it as a zero-cost basis item, and only pay tax when you sell it. The more conservative treatment is to treat it as income as it hits your wallet (either looking at the balance in the staking contract or when you claim it) – your tax authority wants their money, and they want it now – deferring is usually a more aggressive stance. But, as always, talk to your tax professional. Your mileage might vary.
This applies to various forms of deposit contracts – Yearn / Harvest vaults, Compound / AAVE deposits, and other instruments that look and smell like interest-bearing accounts.
But, what about something tricky that I know everyone is thinking about – ETH 2.0 staking? Well, that is a lot more complicated. Because you can only deposit into the ETH 2.0 contract right now, and because there’s no concrete plan to enable withdrawals, and it’s up to a bunch of random people with GitHub screen names – this really feels like a non-callable loan. Like a loan to your sister-in-law, you can hope it gets repaid, but you shouldn’t be counting on it. Talk to your tax professional about how to treat it, but many tax professionals in the crypto space are saying not to recognize any of the ETH 2.0 staking rewards until you can actually claim them.
NFTs: THE SLIPPERY SLOPE OF THE DeFi SPACE
We’ve tackled liquidity pools, we’ve tackled staking and yield farming – how about NFTs? Well – this one is tricky. At a high level, they are an asset like anything else on the blockchain – you want to treat the acquisition of an NFT like other assets (see how we treat multi-asset transactions, for instance, if buying the NFT took some tokens, some WETH, and cost some fees).
But here’s where things get complicated – in the United States (and several other tax jurisdictions), collectibles are taxed differently than stocks and bonds. That is to say, they generally don’t have long term capital gains treatments. What does that mean for you?
Well, and I’m sounding like a broken record, but talk to your tax professional.
The treatment comes down to intent and use – did you buy a Steph Curry TopShot because he’s your favorite player and you loved the 3-pointer he was draining? That feels a lot like collecting. Were you putting money into a crypto bond to earn a yield? Not so much collecting (though, some crypto bonds have really pretty digital designs, which definitely starts to muddy the waters). It gets even more tricky if you’re a business that’s actively trading NFTs, that feels more like normal business operations rather than collecting, but boy does it get gray. Tax professionals are your friends in this chaos!
Finally, if you’re creating NFTs to sell, and selling them for a profit, that’s just like any other artist and you probably need to pay income taxes on them. My third cite below is a link to DeFi crypto experts to help you along your path.
There are some things I haven’t covered (like lending pools, how to record losses from hacks, and what to do about token vesting periods), but this should get you started down the path of paying your taxes. And please remember – pay your taxes and be honest with the IRS.
Usually, tax resistance is futile. If you decided to buck the system people receive letters from the IRS stating they owe funds. Also common: having 15% of their social security check or employment check garnished every month to pay the tax debt. More recently, with crypto IRS debt, if someone has a significant tax debt (over $50,000) they may not be allowed to renew their passport. The IRS knows crypto investors can move their fortunes easy without being detected.
Which brings us to the last taxing question: Do you know about tax havens?
There are roughly 195 countries in the world and almost 25% (45) of them are considered tax-havens. The more popular tax-havens most people are familiar with are the ones located on small tropical islands, such as the Cayman Islands, Bahamas, St. Martin, St. Lucia, Seychelles, Turks and Caicos, and Bermuda.
There are the lesser-known tax-havens located in key business hubs such as Hong Kong, Panama, and Singapore.
There are also tax havens in well-established and developed countries like Ireland, the United Kingdom, and the Netherlands.
Two jurisdictions worth mentioning for cryptocurrency enthusiasts are The Republic of Malta and Panama. They offer some interesting options for people. Research them.
You can now set up an offshore haven easily with the help of a new company, Korporatio. Blockchain is a perfect ‘use case’ for recording and storing incorporation filings and one such company that has taken this to task is Korporatio, which offers blockchain incorporation for various off-shore jurisdictions starting at just $1,000. Research them to learn about how to use the rules to favor yourself.
Again, here is the hyperlink for my crypto tax software.
The take home from the IRS: Don’t sell your crypto if you don’t have to because no taxes become due.
I buy my crypto by depositing USD in the Gemini/BlockFi exchange because they have the low transaction charges. Then I send the crypto assets to my wallet.
For context: Some vegan ex neuroscientist tried to get on stage and tell me that quantum mechanics has no role in biology. He made and ass of himself and I was happy to see him do it. First it highlights the limitations of critical thinking on a vegan diet. Two, it explains why he is an ex scientist. He failed at critical thinking.
Anyone who tells you quantum entanglement is not operational in Nature needs to be reeducated.
@PaulCapestany is the vegan ex neuroscientist who came on stage in Dennis Porter’s room today and try and dox me. Here is the paper to refute his premise. There are hundreds more and books like “Life on the Edge” by Jim Al Khalili that show you the depth of his educational arrogance.
Nature provides “a why” for things to live, and as such, living things can bear almost any how the Earth can throw at it. So this raises the difficult question: why don’t humans understand magnetism well? When you have no framework of understanding a topic, a question of why is fruitless. This is counterintuitive to most and it is one of the ways a skeptic undresses themselves by showing their ignorance. Scientists are an interesting breed of people, they are creative, adventurers, critical, and pragmatic. This may not be the initial subset of people you would look to for inspiration. However, think for an instance of the motivation required to tackle the great intellectual challenges of our time. Scientists are driven by constant curiosity and inspired to find truth. Physicians should be too, but the paradigm today is not about truth, it is built around following evidence they believe on the menu for health. Magnetism rarely comes up as a topic for wellness in any office. That is unfortunate. Paul tried to bring it up in ClubHouse today but he was so ignorant he had no idea how the brains mitochondrial creates its own magnetic field because of the rotating F0 ATPase head that contains an electric current. Micheal Faraday show the experiments in physics that proved this happens in the 1800s. James Clerq Maxwell used mathematics to prove Faraday correct. Today we have MEG machines for the brain and heart that show us our colony of mitochondria create magnetic fields in biologic systems that we can impact with our choices.
The problem with people like Paul is not their ignorance of new data. The issue is being educated just enough to never question what you were taught in the first place. I even volunteered to give him the data points to study and he was not interested in the least.
What’s even most frustrating is when you literally give someone like Paul the ex-neuroscientist, the resources to solve their Dunning Kruger moments, but they are unwilling to put the effort in to educate themselves. That is pathetic.
No scientist was more interesting than Feyman, in my opinion, because of how he understood nature. Examining nature from his perspective is how I think about her laws. “Two things are infinite: the universe and human stupidity; and I’m not sure about the universe.”
The “mitochondriac clinician” should be known by having chosen to clash with popular thinking and the limited imagination of fellow scientists, clinicians and the public if we are to ever advance our knowledge in biology. It is not a popular place to be, but it is the position where ultimate truths will be revealed, in my opinion. This situation does not bother me as a clinician today. I realize my professions’ limitations currently, but I am driven to push the boundaries of what is possible for patients by understanding how magnetism affects our cells. The history of medical discovery has taught me to be patient. For me it was once strange to realize that the history of medicine is littered with stories of extraordinary people who made novel discoveries by asking a question nobody else thought was worthwhile. Moreover, with time, the world usually seems to awaken to new realities in understanding, and it then appears so easy and simple for anyone to accept. The history of science is saturated with stories like this.
What nature does not forbid…….most certainly will happen eventually. That really is the story behind biological evolution, but not too many see it my way, yet. Our beliefs are still tethered to natural selection by convention. It follows that in nature and human imagination, anything is possible, and this is why, in nature, there is no law except the law of nature that there is no law.
The problem is not people being uneducated; the problem is that they are educated just enough to believe what they have been taught, but not educated enough to question what they have been taught. It’s easier to fool people “using choice controls” than to convince them that they’ve been fooled. Who comes up with diagnostic criteria anyway? The paradigm does in healthcare. Who does this on social media? In technology, it’s the tech industry. If you control the choice you control the game. This is why FB has no dislike buttons. In case you’re wondering why things built for profit use this ideology, all one needs to do is realize it is a giant sales funnel. It’s a profiteering scam. Whoever names the game by controlling choices and options, owns the game. This is why the government wants control of healthcare too.
That’s why mitochondriacs focus on the most fundamental layers of physiologic function: light water and magnetism. It is also why functional medicine practitioners focus on bio-chemical pathways: It drives their profits through their testing and supplements. This is how they make money. It is time for you to realize that wake up call. Now we have functional medicine types using healthcare and technology platforms to really control choice of their customers. They are now using both together.
Consider the technology shell game they employ. When using technology, we often focus optimistically on all the things it does for us with their products. But I want to show you where it might do the opposite effect on our biology.
Where does technology exploit our minds’ weaknesses?
I learned to think this way when I studied to become a magician as a kid after I saw a magic show at a birthday party. Magicians start by looking for blind spots, edges, vulnerabilities and limits of people’s perception, so they can influence what people do without them even realizing it. Once you know how to push people’s buttons, you can play them like a piano.
And this is exactly what product designers do to your mind. They play your psychological vulnerabilities (consciously and unconsciously) against you in the race to grab your attention.
I want to show you how they do it.
Hijack #1: If You Control the Menu, You Control the Choices
MEDICINE’S MENU FOCUSWhat is not on the menu but
Should be? MAGNETISM
Great Option #1
Great Option #2
Great Option #3
Western functional medical culture is built around ideals of individual choice and freedom from the “constraints of allopathic medicine”. I chuckle when I hear the profiteers speak this way. They use the techniques far better than allopathic medicine does. Millions of us fiercely defend our right to make “free” choices, while we ignore how those choices are manipulated upstream by menus we didn’t choose in the first place. Is medicine’s menu the same one nature used to built wisdom in our cells? Have you ever thought about health in this way?
This is exactly what magicians do to people. Many people throughout history have mentioned that when you examine and look at quantum mechanics, it defines what magic really seems to be. This is the science that forms the basis of reality and all nature and we ignore it. Magnetism is part of nature’s magic used in every cell. People like Paul have no idea how factual this statement is.
Using magic trick for your audience is way easier when your target audience has lowered dopamine level in their neural networks. This is often why hospitals, offices, and casino’s favor artificial blue light frequencies to illuminate environments for the customers. It makes people more docile and easier to control for the profiteer. Blue light lowers magnetic flux in our mitochondria. Paul believes bursting on the scene in ClubHouse can mimic a casino. It cannot because my job is to educate you about people like Paul. This is not how people understand magnetism, so that is why they do not understand the why of magnetic effects of different light frequencies on their mitochondria. In a magic show, magicians give people the illusion of free choice, while architecting the menu so that they win, no matter what you choose. I can’t emphasize enough how deep this insight is when viewing how paradigms operate today.
When people are given a menu of choices, they rarely ask:
1. “what’s not on the menu?”
2. “why am I being given these options and not others?”
3. “do I know the menu provider’s goals?”
4. “is this menu empowering for my original need, or are the choices actually a distraction?” (e.g. an overwhelmingly choice of supplements for example)
For example, imagine you’re out with friends on a week day night and want to keep the conversation going. You open the “Yelp App” to find nearby recommendations and see a list of bars. The group turns into a huddle of faces staring down at their phones comparing bars. They scrutinize the photos of each, comparing cocktail drinks. Is this menu still relevant to the original desire of the group?
It’s not that bars aren’t a good choice, it’s that Yelp substituted the group’s original question (“where can we go to keep talking?”) with a different question (“what’s a bar with good photos of cocktails?”) all by shaping the menu. This change went below your perceptual abilities because it was done over blue light and a network built of nnEMF. Both are designed to lower magnetic flux in your mitochondria to lower ATP levels to get you to choose what is good for them and not good for you. This lessens our ability to think well. It is part of technology design.
This is what a vegan diet does to human cortex. The ATPase cannot spin at its highest rate to support cognition in superior fashion. Do you think Paul knows this?
Think about the video above now. Feyman had difficulty telling his interviewer why magnets do as they do. In my example above, you all have had this experience to understand the framework. None of you realized it was tied to magnetic flux in your mitochondria by the use of light frequencies.
Will this change how you understand how aberrent light frequencies can affect your life?
That is for you to decide.
Let us go back to the Yelp App to make the point clear.
Most people in our group example falls for the illusion that Yelp’s menu represents a complete set of choices for where to go. Is this like what happens in a doctors office or a hospital? The ER? In a grocery story? At college? At your bank or brokerage house? I think it is. The reality of this situation is that when people are looking down at their phones, they don’t see the park across the street with a band playing live music. They miss the pop-up gallery on the other side of the street serving crepes and coffee. Neither of those show up on Yelp’s menu. Do they mention bitcoin or just assume you’ll pay in fiat? What isn’t on your health menu where you spend you medical dollars?
There is a pardox of choice………only when we know there is other choices. So what do healthcare and technology paradigms use in common to win?
They control the choices by controlling the menu of what they think you should know, want or ask.
This is precisely what has happened with COVID. They assume everyone will want a vaccine after a lockdown for year and they are stunned that vaccine hesitancy exists. Sometimes vaccine hesitancy can lead to a divorce in a relationship.
The more choices technology or healthcare gives us in nearly every domain of our lives (information, currency, events, places to go, friends, dating, jobs) — the more we assume that our phone is always the most empowering and useful menu to pick from. Is this really factual? Is it based upon nature’s laws of engagement for cells?
The “most empowering” menu is different than the menu that has the most choices. Nature provides cells with all options. It is a decentralized network. All things that at decentralized are thermodynamically most efficient by quantum laws.
The only man made decentralize network I have found in six decades is Bitcoin.
In fact, it gives cells options they are not even optimized for, but they can use them if they change things. This is what evolution is all about. Nothing is off the table given the environment on Earth powered by sunlight. But when we blindly surrender to the menus or currency we’re given in the modern tech world, it’s easy to lose track of the difference in outcomes:
“Who needs their gallbladder removed” becomes a menu of the things published as evidence in a textbook
“Who’s free tonight to hang out?” becomes a menu of most recent people who texted us (who we could ping).
“What’s happening in the world?” becomes a menu of news feed stories from social media.
“Who needs a vaccine” becomes a menu or algorithm set in place by the CDC or government.
“Who only believes fiat is a store of value and a unit of transfer?”
“Who’s single to go on a date?” becomes a menu of faces to swipe on Tinder (instead of local events with friends, or urban adventures nearby).
“I have to respond to this email.” becomes a menu of keys to type a response (instead of empowering ways to communicate with a person).
To every thing there Is a season, but with sunlight there is always some type of modulation that slightly varies its power to allow time to manifest. This is how nature creates a specific variety of frequencies (and magnetic flux) that our cells are rewarded by. Innovation favors the connected life. The functional medicine doctors will never get you to this level because it removes the variable rewards they need to thrive in their business. This problem is not just one in allopathic medicine. I believe it is greater issue in functional medicine. Why? Their framework is less understood by the public than allopathic medicine so people rely on their menu of choices even more. This is why the “bulletproof selection” menu is devastating to many. What are some of those menu choices doing to us? Sales of supplements and tests that give partial or variable successes are hugely powerful tools to those involved in the functional medicine business. Vegans do this to with supplements. How good can your dietary choice be when you need supplementation to maintain health or your ability to think?
Why do they do this? The functional medicine paradigm learned this from studying gaming. They are in a game to try to usurp the power of allopathic medicine. So they shrewdly went to look at how casino’s separate us best from the money in our wallets.
One major reason why is the #1 psychological ingredient in slot machines: intermittent variable rewards.
If you want to maximize addictiveness (a lowered dopamine effect), all functional medicine needed to do was study what technology designers did in casinos and in Apps we use. Their business plans only need to link a user’s action (like pulling a lever) with a variable reward attached. If you don’t believe it just sign up for the emails of the “bulletproof executive” for a month and tell me if you do not see this post in every email you get.
The media world today is enveloping man in bullshit. This is especially true in the financial world with Bitcoin deceit uttered by the old vanguards of capitalism who support the Federal Reserve = Charlie Munger & Warren Buffet. It is no surprise neither support BTC. Charlie and Warren own banks that launder billions per year and have been charged criminally. Give me a break. It reminds me of Upton Sinclair comment: “It is difficult to get a man to understand something, when his salary depends on his not understanding it.”
His views are not based on knowledge or research – his views are instead an expression of his inability to grasp new concepts, new frontiers and new technological innovation. Not because of his age necessarily – its his attitude where the problem lies. Paul Capestany, Warren, and Munger all share the same deficits in critical thinking for different reasons.
Some of the misinformation shared is intentionally designed to deceive, and some of it is mouthed by people too ignorant or frightened to distinguish natural truth from falsehood. I think Paul Capestany of ClubHouse fame represents the latter.
Having an open mind is critical in being a mitochondriac, but we all need to remember in today’s social media empire, having an open mind with no framework of natural understanding, will allow people with profit motives to come in and put many things in your head. Be mindful of this.
DOCTORING:
Doctor = teacher who uses words, not prescriber. Empowering patients to be informed people and not blind sheep is a sign of a great teacher.
You can lead people to water, and though you can’t make them drink, you *can* give them the awareness that they’re’ thirsty.
That is my post mortem today from ClubHouse. We have to call out the bull shit artists among our tribe. They can decide who is right and who is wrong.
Red, itchy eczema patches may look contagious, but they’re not. Eczema is basically an altered immunologic disease in the skin that starts out as an itch that turns into a red rash. The itch of eczema can be hard for others to understand. Patients with this disorder say it can feel like poison ivy, chickenpox, and a sunburn rolled into one skin condition.
The skin can also get rough and scaly, with sores that ooze and crust over. To manage the symptoms, some alternate between taking Epsom salt baths and showers. That is what most physicians tell their patients because that is what is taught in medical school. Those answers do nothing to get rid of the disease. They only treat the symptoms on a short term basis.
The answer to reversing the disease is getting solar exposure more frequently to properly program the T cells in your skin to raise the melatonin levels in your skin. No one learned this in medical school.
Reality alert = Is eczema an allergy to nnEMF or blue light toxicity?
It might be. Read the below carefully. Is sunlight a wireless vaccine that can help this condition? It might be. Sunlight has so many benefits I might have written volumes about its effect. There are so many hidden benefits people don’t just get because people are taught these days to bury the sun by my profession. This is an example of how a centralized curriculum in medical school is really an analogue algorithm of a by gone era.
We, like trees, need physiologic solar exposure. For me, I use it to reduce my overall nnEMF/blue exposure I get in surgery and in my life; in addition, it has massive effects on dopamine, serotonin, histamine, melatonin, sulfation, methylation, and Vitamin D3, gut biome populations, charging my exclusion zones up by raising my DC electric current to lower the work my mitochondria needs to do. No area is difficult to get sun on if you just expose your skin to the problem region. The results of that “wireless vaccine” of light might shock you!!! That is why eczema remains a large problem today. People cover up far too much. If you child has eczema it maybe that pre-pregnancy and during pregnancy your body did not get enough sun and this altered your T cell cells in your skin. We have more T cells in our skin than in any other organ. When this occurs this information can be epigenetically transferred to your child via mRNA signaling to change the childs’ skin physiology. This condition might be a baseline acute immune reaction of a de-programming of T-regulator and helper cells from a lack of sunlight!!!!!
STATIC SHOCKS AND ECZEMA
Most people are familiar with electrostatic forces that are weak. Examples of weak electrostatic force is when humans rub a balloon and the hair on their body stand up on ends or what that some materials, such as amber, attract lightweight particles after rubbing.
Usually insulators, e.g., substances that do not conduct electricity, are good at both generating, and holding, a surface charge. Some examples of these substances are rubber, plastic, glass, and pith. Conductive objects only rarely generate charge imbalance except, for example, when a metal surface is impacted by solid or liquid nonconductors. The charge that is transferred during contact electrification is stored on the surface of each object.
Skin is actually a very good insulator as well so, relative to metal, humans aren’t very good conductors. Because the skin is a good insulator it means Nature engineered it to hold electric charges from sunlight for some reason. What might those reasons be?
Sunlight create electric fields in our atmosphere every day and that sunlight creates a Coulomb force. Coulomb force is an electrostatic force. Electrostatic phenomena arise from the forces that electric charges exert on each other. Such forces are described by Coulomb’s law. Even though electrostatically induced forces seem to be rather weak because of how we experience them in life, when the scale shrinks, as it does in a cell, the electrostatic force increases tremendously in its power. For example, some electrostatic forces such as the one between an electron and a proton, that together make up a hydrogenatom, is about 36 orders of magnitude stronger than the gravitational force acting between them. The electrostatic force generated in your skin is another example of a strong electrostatic force because the skin, as an insulator can hold large amounts of charge.
People are unaware that this force involved with the biology of melatonin and the function of mitochondria where electrons and protons are the target of this force because they are charged particles. The same thing is true of T-Regulator cells in the skin.
Although charge exchange happens whenever any two surfaces contact and separate, the effects of charge exchange are usually only noticed when at least one of the surfaces has a high resistance to electrical flow. An alteration in the electrical charge in your skin is one of the major reasons why many people cannot convert cholesterol containing semiconductors in their skin to 25-D-OH Vitamin D. Tattoos also alter the charge state of the skin because of the atoms in the ink.
This is because the charges that transfer are trapped there for a time long enough for their effects to be observed. These charges then remain on the object until they either bleed off to ground or are quickly neutralized by a discharge: e.g., the familiar phenomenon of a static “shock” is caused by the neutralization of charge built up in the body from contact with insulated surfaces. With melatonin, T Cell functioning, and skin physiology the charge are rarely seen because charges are transferred to electrons and protons in the chemicals of cells.
Coulomb force, also called electrostatic force or Coulomb interaction, is the attraction or repulsion of particles or objects because of their electric charge. When people get skin outbreaks the charge within the epidermis is a manifestation of charge discharge in the skin. This is analogous to the static discharge mentioned above. The redden plaque is the manifestation of a charge transfer problem in the skin. When electrostatic force cannot be discharged properly it can effect Gauss law in our body. Gauss’ law states that “the total electric flux through any closed surface in free space of any shape drawn in an electric field is proportional to the total electric charge enclosed by the surface. Since a mitochondria is a close organelle that contains massive amounts of electrons and protons at a small scale any altered discharge of an electrostatic field causes a change in Gauss’s law with respect to the mitochondria. What is this a big deal?
Mitochondria make water, CO2, and melatonin. Melatonin, doc? Yep. We now have very new data that shows that mitochondria make the chemical that regulates its ability to transform energy in tissues locally.
This recent paper describes this finding. We now know mitochondria synthesize and release melatonin. This occurs via their selective G protein-coupled receptor (GPCR) in the outer membrane of the mitochondria. The paper demonstrated that mitochondrial melatonin type 1 receptors respond to melatonin by activating circadian coupled G proteins located in the intermembrane mitochondrial space. These proteins, once powered up by the redox potential created in the power plant than become able to inhibit stress-mediated cytochrome c release. Cytochrome C controls water production in the mitochondrial matrix from metabolism and it control autophagy and apoptosis programs in mitochondria which link it to redox power. Nature’s use of this unique wiring mechanism gives mitochondrial educators insight to how we need to changes our thinking about how humans operate. The classical understanding of biological GPCR function, taught in a centralized medical curriculum is OUTDATED badly. This has huge implications for how we should be treating diseases. The new data is telegraphing us that the powerplant of a cell has the ability to synthesize and act as a signaling receptor for a specific ligand. This ligand is likely tied to the circadian mechanism of the peripheral clock genes present in tissues. This means the wiring diagram shows mitochondria come built in with a automitocrine signal which creates melatonin locally to prevent degeneration and disease by limiting the downstream effect of cyctochrome C release on caspase activation. Caspases are a family of protease enzymes playing essential roles in programmed cell death.
Why is this a big deal? We know that melatonin deficient tissues are more likely to develop cancers. We also know that caspase deficiency has been identified as a cause of tumour development. This paper now makes the link between these two concepts and explains why skin diseases are harbingers of future cancer risk.
Early mitochondrial damage shows up in people with Hay Fever & Asthma
People with loss of redox power in their immune systems tend to get mitochondrial diseases earlier in life. This is why there is a connection between those two conditions and rosacea and atopic dermatitis. If a parent has hay fever or asthma, their children are more likely to have the skin condition. And many children with atopic dermatitis will go on to get hay fever and/or asthma.
Most often the cause of these disorders are due to a change in the semiconductive properties of the skin and the reason is often tied to our light environment. When light hits a semiconductor a DC electric current result in tissue. We can measure with with surface electrodes and an oscilloscope. Electric charges cause electromagnetic force fields around them. This causes things to do the things they do = physiology of the tissue in question. When the semiconductor in the system is defected the phenotype of the disease manifests. That is what causes eczema plaques.
Phototherapy:
UV light affects the immune system. In some people, it can improve moderate to severe cases of eczema from atopic dermatitis, rosacea, or contact dermatitis. Usually, these treatments use UVB light. “PUVA” is a UV treatment combined with a drug called psoralen. I do not like the drug, so I replace it with photobiomodulation and this improves clinical efficiency in therapy. Skin docs use UV light in an artificial manner by itself. UV is never present from sunlight without the other frequencies of visible light. This is why I balance the huge Coulomb force created by UV light with red light.
Coulomb forces must be balanced after daytime and this occurs at night when light is absent. This is why light at night is so bad for us, and why a centralized doc has no ability to figure out why this occurs. It is also why your dermatologist has no clue to the cause of eczema. You have to understand how Coulomb’s force becomes unbalanced to alter how mitochondria can transform energy. That break in the pathway is the charge on melatonin in the skin which affects the mitochondria in the skin to give a person eczema. Melatonin in mitochondria of tissues are created by the Coulomb forces in AM sunlight. Melatonin levels vary within tissues because of how much light tissues get. As a result, it appears melatonin is a guardian of the Mitochondrial genome (37 genes). Out of the 37 genes, 13 of them are specific to energy-transforming mitochondrial genes. Those 13 genes only code for the proteins that tunnel electrons and spit protons out of the mouth of cytochrome proteins. The mitochondrial genome undergoes 3 times as many genomic mutations as the nuclear genome by design. Melatonin levels are critical in monitoring mitochondrial behavior and light energy transformation by controlling how energy is being transformed from light to create physiologic power.
The major function that melatonin helps smooth-out in mitochondria are
Energy metabolism and flux via control of electron and proton tunneling.
Redox balance within the mitochondria = GSSH (glutathione)
Ion homeostasis = electrostatic controls via Coulomb forces that vary via light
The signaling of cell death and mitophagy = % heteroplasmy in a mitochondrion = the amount of melatonin your skin makes from its mitochondria = the amount of light energy transformed to physiologic power in the skins component semiconductors.
How Light Treats Acne
Acne forms in pores — the tiny holes in your skin. Each pore contains an oil-producing gland. The oil keeps your skin healthy.
But sometimes the oil, dirt, and dead skin cells can get trapped inside pores and clog them up. Bacteria called Propionibacterium acnes (P. acnes) that live on your skin can also get inside these blocked pores. P. acnes make the clogged pores swell up into bumps called acne.
One way to kill bacteria and clear up pimples is with light. The bacteria in your skin are sensitive to certain types of light. When you shine these lights on your skin, toxic substances form and kill the bacteria. Light therapy also shrinks the oil glands in your skin, so your skin makes less pore-clogging oil.
Doctors used to treat acne with ultraviolet (UV) light. The smart play is to use full spectrum sunlight to help acne or cystic acne because sunlight has red light in it that help resolve the inflammation in the follicles.
You may get special medicine before your treatment to make your skin more sensitive to the UV light. Doctors call these medicines “photosensitizers.” They include aminolevulinic acid (ALA) and methyl aminolevulinate (MAL). The smarter play is to use red light therapy to precondition the skin to absorb more UV light and you won’t need the drugs to deal with the acne.
This is why docs cannot solve many skin diseases, but sunlight can and does. A lack of sunlight or excessive blue or nnEMF causes many skin diseases.