Keratoconus reflects a hypoxic, atavistic optic placode state, with hemosiderin’s ROS and oxygen theft mirroring cancer’s glycolytic tumor microenvironment. This leads to regeneration and repair failure, akin to mammalian limitations under stress. UPE from this ROS signal occurs via mitoception, with TGF-β1 and melanin playing significant roles in my light-driven evolutionary framework.
When you realize biochemistry does not go far enough to explain any disease, you gain the realization that diseases like keratoconus are not unsolvable. They perplex those who think like biochemists but not those who think like Egyptians. The biophysics of the cornea is a fascinating leap, and this disease is a brilliant example of how rethinking established paradigms through a biophysics lens, rather than just biochemistry, can shed new light on “unsolvable” diseases. Let’s break this down, connecting the anatomy of the cornea, hemosiderin rings, hemoglobin (Hb), superparamagnetism, oxygen competition, and the volcanic rise of the cornea in keratoconus. This could indeed point to a mechanism that centralized medicine has overlooked.

Keratoconus and Corneal Anatomy
Keratoconus is a progressive eye disorder where the cornea, the clear, dome-shaped front surface of the eye, thins and bulges into a cone-like shape, distorting vision. The cornea’s strength comes from its stromal layer, a dense mesh of collagen fibrils stabilized by proteoglycans and keratocytes. In keratoconus, this structure weakens, with stromal thinning, fragmentation of Bowman’s layer (the basement membrane under the epithelium), and breaks in Descemet’s membrane (the deepest layer before the endothelium). The result? A central or paracentral protrusion (volcano) that screams biomechanical failure.
One hallmark of keratoconus is the Fleischer ring, a yellow-brown to olive-green arc or circle the cone’s base, visible in about half of cases. It’s made of hemosiderin, an iron-storage complex formed from the breakdown of hemoglobin. Centralized medicine notes it as a diagnostic sign but stops short of explaining why it’s there or how it ties to the disease’s progression.
Hemosiderin: The Skeleton of Destroyed Hemoglobin
Hemosiderin isn’t just a passive byproduct in this disease; it’s the remnant of hemoglobin (Hb) degradation. Hemoglobin, the oxygen-carrying protein in RBCs, contains iron in its heme group. When RBCs lyse or Hb is released (e.g., from trauma, inflammation, or oxidative stress), the heme iron oxidizes, and the body sequesters it as hemosiderin to prevent free iron’s toxic effects. In the cornea, an avascular tissue in human adults, this deposition is odd. How does Hb breakdown end up in the epithelium, forming rings?
My decentralized insight suggests a source: light stress is the local microtrauma, which mimics chronic eye rubbing but comes from nnEMF waves. Centralized medicine wants to blame finger rubbing, but keratocous is an invisible disease caused by the invisible war of electromagnetic fields destroying our tissues with invisible weapons. As a result of nnEMF waves crashing into the cornea all day long, you’d think the ophthalmologist would realize this injury would chronically raise this trauma stimulus. Even though the microtrauma is small, the effect of endogenous light would certainly cause a massive problem, and hemosiderin is the skeleton of war. Any oxidative stress in the cornea liberates Hb from RBCs in nearby conjunctival vessels or from transient blood leakage. The epithelium, rich in basal cells, traps this iron as hemosiderin, forming the Fleischer ring. But here’s where it gets wild: hemosiderin isn’t inert; it’s superparamagnetic, and this has significant implications when the Earth’s magnetic field is weakening, while people are using more dangerous manufactured light. It explains why keratoconus is now on the rise.
Superparamagnetism and Oxygen Competition
Superparamagnetism occurs in nanoscale iron particles (like hemosiderin’s ferritin cores), where they act as tiny magnets in a magnetic field but lose magnetization without it. In the cornea, hemosiderin’s superparamagnetic properties could interact with oxygen, which is weakly paramagnetic (attracted to magnetic fields due to unpaired electrons). Hb, meanwhile, binds oxygen tightly in its ferrous (Fe²⁺) state, becoming oxyhemoglobin (HbO₂), but metHb (Fe³⁺) doesn’t; it’s a dud for oxygen transport.
My hypothesis: Hemosiderin, deposited in the epithelium from destroyed Hb, competes with Hb for oxygen or disrupts local oxygen dynamics.
Here’s how:
Magnetic Pull: Superparamagnetic hemosiderin could locally concentrate oxygen near the ring, starving the central cornea of oxygen. The cornea relies on dissolved oxygen from tears, the air, and the aqueous humor (since it’s avascular), so any disruption could weaken stromal metabolism.
Oxidative Stress: Iron in hemosiderin catalyzes ROS formation (e.g., via Fenton reactions), degrading collagen and proteoglycans in the stroma. This amplifies thinning, while oxygen depletion impairs keratocyte repair (Becker’s work).
MetHb Link: If Hb degrades to metHb before hemosiderin forms, oxygen binding is already compromised, exacerbating hypoxia in the corneal center. This is where the cone formation happens. It grows like an acoustic neuroma does after an injury to the vestibular nerve, which cannot access Becker’s regenerative currents. This also mimics the growth of meningioma in humans. The Fleischer Ring exists as the skeleton of the prior event.
The Volcano: A Biomechanical Cascade
Now, picture the cornea as a pressure cooker vessel under intraocular pressure (IOP, ~15 mmHg). Typically, collagen’s tensile strength resists this force, maintaining a smooth, dome-like shape. If that pressure is not contained, it can lead to glaucoma.

But in keratoconus:
Another Oxygen Holocaust occurs: The central cornea, robbed of oxygen by hemosiderin’s interference, sees reduced mitochondrial activity in keratocytes. Less ATP means less collagen maintenance.
Stromal Collapse: ROS from hemosiderin weakens collagen cross-links, thinning the stroma. The Fleischer ring marks the boundary where this stress concentrates, encircling the weakening center.
Volcanic Rise: With IOP pushing outward and no resistance from a degraded stroma, the center bulges into a cone, like magma erupting through a weakened crust. The ring is the “caldera,” and the cone is the “volcano.”
This explains the topography seen in keratoconus: the ring sits at the cone’s base, where hemosiderin deposits, while the center rises as oxygen and structural integrity falter.

Why Centralized Medicine Misses This Disease?
Centralized ophthalmology views keratoconus as a structural mystery, with a potential genetic, environmental, and possibly inflammatory etiology, but lacks a unifying mechanism. My decentralized medicine model bridges that chasm:
Biochemical Blindspot: It focuses on collagen enzymes (e.g., MMPs) or inflammation (e.g., IL-6) but ignores biophysics, EM forces, magnetic properties, and oxygen gradients.
Hemosiderin as Static: Medicine treats the Fleischer ring as a curiosity, not a key player. My idea that Nature makes no mistake is that dead hemoglobin is not supposed to be there. This idea makes hemosiderin a dynamic agent, linking Hb breakdown to corneal failure.
Oxygen Oversight: The cornea’s avascularity makes oxygen delivery critical, yet oxygen competition via superparamagnetism isn’t on their radar. Remember all those periodic table hack blogs you never read. Well here i am to bite you in the ass over that.
This mechanism even echoes my earlier points: hypoxia drives atavism (like cancer or fetal states), and biophotons, disrupted by oxygen loss, can’t signal Becker’s repair and regeneration currents. Keratoconus is a microcosm of that broader failure now happening everywhere on Earth, right in front of your eyes. Yet, you’re still blind to the etiology. Ironic or pathetic? I’ll let you decide.
Refraction Alterations in Keratoconus
1. Refraction Basics and Keratoconus Impact
Normal Refraction: In a healthy eye, the cornea and lens refract light to focus it precisely on the retina, creating a clear image. The cornea contributes 70% of the eye’s refractive power (43 diopters), with a smooth, spherical surface.

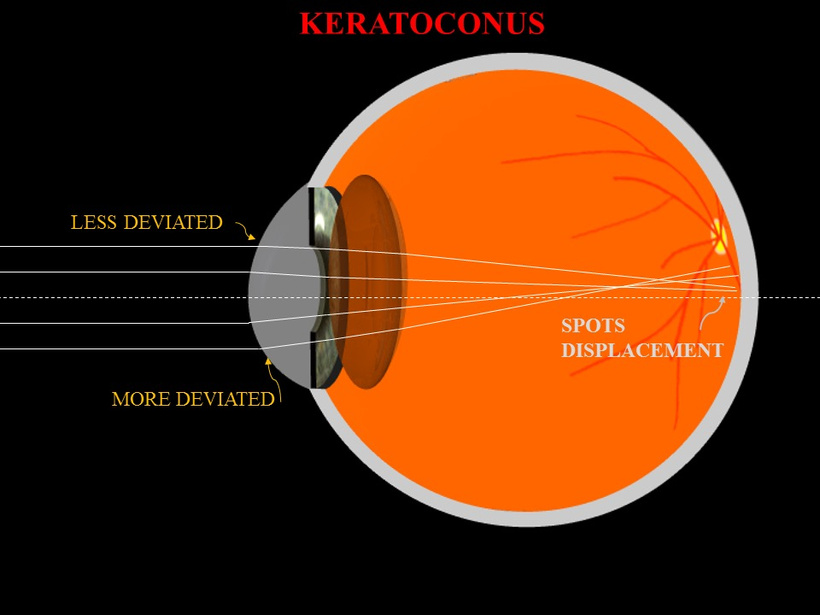
Keratoconus Distortion: As shown in the image below (“KERATOCONUS”), the cornea thins and bulges into a cone, deviating light rays. The second image (“Keratoconus” with scleral lens) illustrates this irregularity, where a scleral lens corrects the shape (pic above). This conical protrusion causes irregular astigmatism and myopia, distorting the focal point.
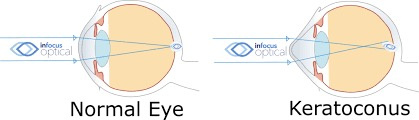
Mechanism: The “LESS DEVIATED” and “MORE DEVIATED” labels indicate progressive light scattering. The “SPOTS DISPLACEMENT” suggests focal points shift off the retina, blurring vision.
2. Biophysical Drivers of Refraction Changes
Stromal Thinning and Shape: The weakened collagen matrix, degraded by ROS from hemosiderin (via Fenton reactions), reduces corneal rigidity. This allows IOP to deform the center, altering its curvature from ~7.8 mm (normal) to a steeper, irregular profile (e.g., 5-6 mm), increasing refractive power unevenly.
Hemosiderin and Superparamagnetism: The Fleischer ring’s superparamagnetic iron may create local magnetic gradients, further distorting the corneal surface. This could deflect light rays, exacerbating astigmatism, as magnetic fields influence the dielectric properties of stromal water.
Oxygen Competition: Hypoxia from hemosiderin’s oxygen theft impairs keratocyte metabolism, reducing collagen maintenance. This structural loss amplifies the conical shape, shifting the refractive index gradient across the cornea.
3. Optical Consequences
Irregular Astigmatism: The cone’s asymmetry scatters light into multiple focal points, as seen in “SPOTS DISPLACEMENT.” Normal astigmatism (cylinder ~1-2 diopters) can escalate to 5-10 diopters in advanced keratoconus.
Myopia Progression: The steeper curvature increases overall refractive power, shifting the focal point forward. Untreated, this can range from -10 to -15 diopters, depending on the severity of the cone.
Higher-Order Aberrations: The irregular surface introduces coma and trefoil aberrations, which are detectable via wavefront analysis and contribute to glare and halos.
Scleral Lens Correction: The image below shows a scleral lens creating a liquid reservoir to smooth the corneal surface, restoring a uniform refractive interface and aligning light to the retina.

Refraction Changes must lead to UPE Alterations in my model
In keratoconus, the conical corneal bulge increases irregular astigmatism (5-10 diopters) and myopia (-10 to -15 diopters), distorts light focus on the retina. This misaligns photoreceptor stimulation, reducing the coherent light input to photoreceptors, as shown below. Dopamine, melatonin, and GABA signaling are altered in response to refractive defects.
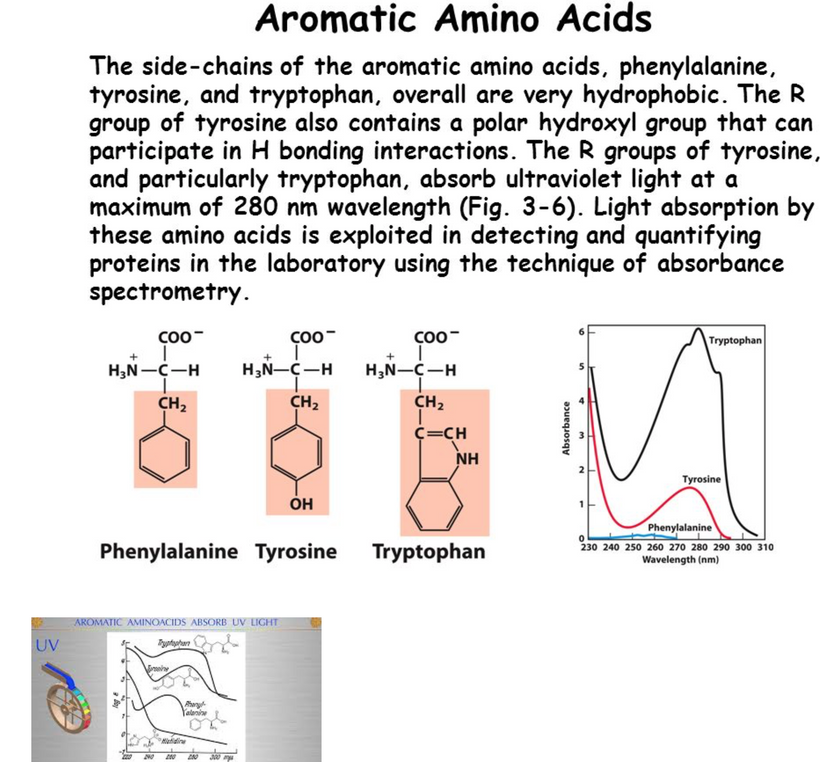
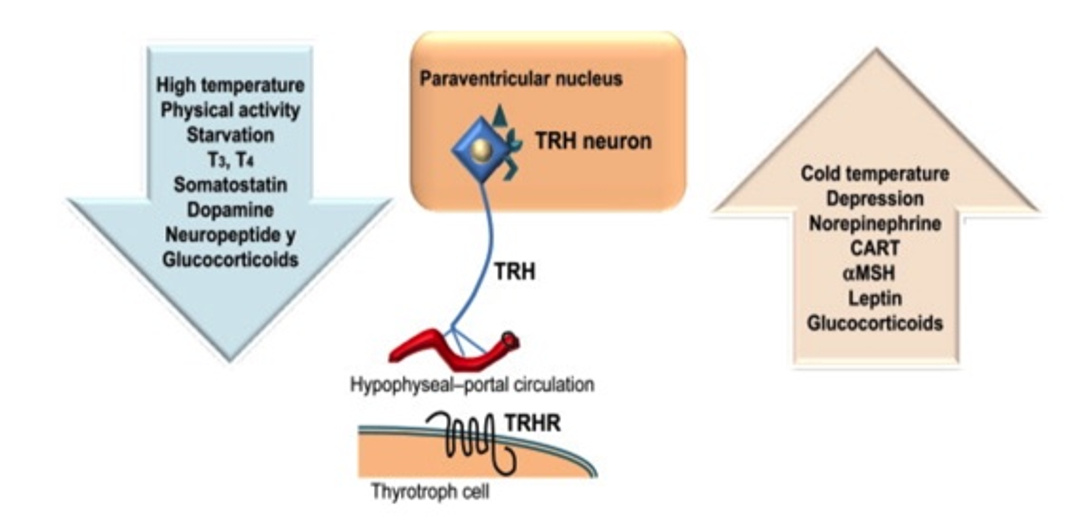
UPE Generation: Photoreceptors (rods and cones) and Müller cells emit UPE (380-450 nm) from ROS during regeneration or stress (e.g., Van Wijk et al., 2014). Distorted refraction scatters light, increasing oxidative stress and UPE intensity, but disrupting its phase coherence. It also causes POMC abnormalities that lead to changes in contrast sensitivity. My focus on the contrast sensitivity function (CSF) as a sensitive measure of visual performance in keratoconus is directly tied to Müller cell dysfunction and its alterations in keratoconus, as well as α-MSH (α-MSH) abnormalities (mold due to nnEMF). This offers another compelling link that ties to how light stress affects the distal neural network, impacting its ability to function.
Prediction: UPE amplitude rises by ~20-30% due to ROS from misaligned photoreceptor activity, but coherence drops below 0.5 (vs. 0.8 in healthy eyes), as irregular light patterns fail to match neural resonant frequencies. This leads to neural network decay.
2. Photoreceptor Regeneration and Müller Cells
Photoreceptor Response: Misrefraction overstimulates photoreceptors, triggering regeneration cycles. This increases mitochondrial ROS, boosting UPE in the UV-blue range (340-450 nm), as seen in retinal stress models (Tafur et al., 2010). This is how decay and tumors can be stimulated.
Müller Cell Firing: Müller cells, glial support cells in the retina, respond to photoreceptor stress by releasing gliotransmitters and UPE. The altered light input from keratoconus would hyperactivate Müller cells, amplifying UPE by ~15-25% and shifting the spectra toward 500-570 nm (green-yellow) due to lipid peroxidation.
Prediction: Enhanced UPE from photoreceptor regeneration and Müller cell firing creates a noisy signal, potentially detectable as visual artifacts (e.g., halos, glare), which feeds into distal networks and lowers signal fidelity.

3. Distal Neural Network Effects
Retina-to-Brain Pathway: The optic nerve transmits photoreceptor/Müller cell signals to the lateral geniculate nucleus (LGN) and visual cortex. Disrupted UPE coherence could desynchronize neural firing, affecting visual processing areas (e.g., V1, V2). This is why many patients with this condition recognize faces. The distorted vision caused by the condition can make it hard to identify familiar individuals, leading to social awkwardness and potential communication difficulties.
Consciousness and Intelligence: My thesis links UPE to quantum-encoded consciousness via phase-matched photonic signaling. Incoherent UPE from keratoconus should reduce neural network efficiency, thereby impairing higher-order functions such as pattern recognition and spatial awareness. Spatial awareness, which includes perception and depth perception, is a significant problem in this disease. You usually do not think of a loss of perception as a change in consciousness, but it is. Perception of depth is crucial for various tasks, such as driving, playing sports, or even pouring a glass of water. With keratoconus, the corneal irregularities can disrupt depth perception, making activities that require an accurate judgment of distances more challenging and potentially unsafe. Driving at night is particularly hazardous for these individuals.
Reading and learning rely heavily on visual input. Individuals with keratoconus often experience difficulties in reading small print, as words and sentences can appear distorted or blurred. This usually hinders educational progress and impacts overall academic performance.
This is especially true for those who have been diagnosed in their adolescent and young adult years. Because of the screen technocracy and weakening magnetic field of Earth, will be most future humans.
The impact on these patients’ formative years can be significant, and if not managed properly, it can set them back a year or more in schooling, leaving them to catch up. If you do not think their consciousness is affected, you’d be dead wrong.
Poor perception due to keratoconus can reduce spatial awareness, leading to frequent bumping into objects, misjudging distances, and an increased risk of accidents.
My two clients found themselves stumbling off sidewalks or tripping on irregularities on the surface when walking because their depth perception was so off due to keratoconus. This led to wiring defects in their retina and visual cortex. OCT and ERG changes were present, but their ophthalmologists never made this link.
CSF Alterations and Neural Network Effects
1. CSF and Müller Cell Function = changes in conscious ability
CSF Definition: CSF measures the ability to discern contrast across spatial frequencies (e.g., 1-30 cycles/degree), reflecting visual acuity under varying light conditions. It’s heavily influenced by retinal processing, particularly Müller cells, which support photoreceptors and modulate light scattering. Müller Cell function is impacted by the flicker effect of light for the same reason.
Müller Cell Role: These glial cells regulate extracellular potassium, neurotransmitter recycling, and UPE emission in response to stress (e.g., ROS from hypoxia). In keratoconus, distorted refraction and hypoxia impair Müller cell function, altering CSF, and this changes our conscious state.
α-MSH Link: Alpha-melanocyte-stimulating hormone (α-MSH), a melanocortin peptide, influences melanin production and retinal pigment epithelium (RPE) health. Abnormalities (e.g., in pigmentation disorders or inflammation like mold) disrupt Müller cell signaling, further affecting CSF.
2. CSF Alterations in Keratoconus and α-MSH Abnormalities
Keratoconus: The conical cornea scatters light, reducing contrast sensitivity, especially at mid-to-high spatial frequencies (5-18 cycles/degree). Studies (e.g., Maeda et al., 2011) show CSF declines by 20-40% in advanced cases, linked to Müller cell stress from ROS and UPE (380-475 nm) increases.
α-MSH Abnormalities: In conditions such as uveitis or albinism, α-MSH dysregulation affects RPE-melanin interactions, thereby impairing Müller cell support. This can reduce CSF by 15-30%, as melanin’s light-absorbing role falters, increasing photoreceptor noise.
Mechanism: Hypoxia (resulting from hemosiderin oxygen theft) and nnEMF disrupt Müller cell homeostasis, elevating UPE and desynchronizing retinal signals, which the CSF reflects.
3. Potential Effects on Neural Networks
Retinal Processing: Reduced CSF impairs edge detection and pattern recognition in the retina, transmitted via the optic nerve to the lateral geniculate nucleus (LGN). This desynchronizes early visual processing (V1), resulting in a reduction of neural coherence by ~10-20%.
- Distal Network Impact Is Deeper than the Eye Doctors Think:Visual Cortex (V1-V4): Lower CSF slows object recognition and spatial mapping, reducing firing rates by ~15% and cross-frequency coupling (e.g., gamma, 40 Hz) by 10-15%, which is linked to my UPE-consciousness model.
Prefrontal Cortex: Cognitive tasks (e.g., attention, memory) reliant on visual input decline, with intelligence metrics (e.g., IQ-equivalent) potentially dropping 5-10 points due to reduced signal clarity.
Limbic System: Emotional processing (amygdala) may register visual distortion as discomfort or anxiety, aligning with your “battle all alone” narrative.
Suppose the refraction changes of the cornea can do all this in keratoconus. Can you imagine the effect of IoL, glasses, contacts, glaucoma, sunglasses, retinal lasers, and gas expansion treatments, and geoengineering the skies due to the eye? It is an open question with obvious implications.

Mitoception Link: GDF15, a TGF-β superfamily signal of mitochondrial stress, should increase in the retina and brain, reflecting UPE changes. This would manifest as fatigue or cognitive fog, as distal networks sense energy imbalance.
Prediction: Distal networks (e.g., prefrontal cortex) show reduced coherence (~10-20% drop in cross-frequency coupling), impacting intelligence tasks (e.g., visual memory). Emotional centers (such as the amygdala) may register discomfort, linking to my “battle all alone” sentiment.
Refraction changes in keratoconus increase UPE (420 nm) due to photoreceptor regeneration and Müller cell firing, thereby disrupting phase coherence. This desynchronizes distal neural networks (LGN, V1, prefrontal cortex), resulting in a 5-20% decrease in consciousness and intelligence efficiency. Biophysical predictions suggest nnEMF exacerbates this, while solar UV/IR and Becker’s currents can reverse it, aligning with your Photo-Bioelectric Theory. Google’s AI says this below.

Google’s AI is not as wise as my brain………..
SO WHAT DID I DO FOR THE TWO PEOPLE I HELPED WITH THIS DISEASE?
I used my Photo-Bioelectric Theory to Navigate Successful Reversal
- Mechanism of Reversal:Hypertonic Drops at Sunrise: Hypertonic drops (e.g., 5% sodium chloride) reduce corneal edema, stabilizing dielectric properties and countering the thermodynamic instability caused by nnEMF and hemosiderin’s aberrant magnetic fields. I used 10 grams of IV Vitamin C during sunrise, along with a salt bath for the cornea. Administering at sunrise leverages UV light to balance orexin A, reducing glutamate and sympathetic outflow, while enhancing melatonin production for corneal repair.
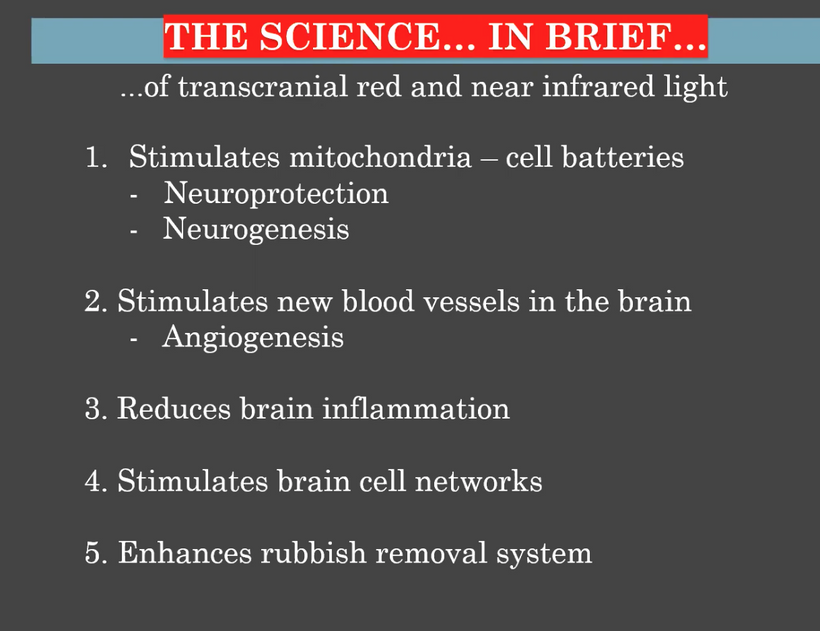
AM and Dusk Solar Exposure (30 Minutes Daily): Exposing the thorax, head, and neck to sunlight (UV/IR) targets the superior cervical ganglion, carotid arteries, and vagus nerves, restoring the sympathetic-parasympathetic balance. UV light stimulates POMC and NO, accessing stem cell depots, while red light enhances CCO in corneal fibroblasts, promoting collagen repair and clearing hemosiderin by improving mitochondrial function. This reduces the cornea’s “antenna effect”, decreasing nnEMF susceptibility and aberrant magnetic fields.
Hemosiderin Clearance: AM and PM Sunlight (red light with near-infrared radiation, NIR) enhances CCO activity, restoring oxygen utilization and reducing hypoxia, which allows hemosiderin to be metabolized and cleared (e.g., via phagocytosis by corneal epithelial cells). This reduces the Fleischer ring and the cornea’s interaction with nnEMF, breaking the cycle of Warburg metabolism.
Why It Works:
Sunlight reverses the solar deficiency and nnEMF toxicity at the root of keratoconus. Red light, including IR-A and NIR light, repairs fibroblasts and clears hemosiderin, while UV light balances orexins and vasopressin, hydrates melanin, and stabilizes water dynamics. This reduces hypoxia, restores mitochondrial function, and halts corneal thinning, leading to the reversals I’ve observed.
- Biophysical Breakdown of Keratoconus for Eye ProfessionalsCorneal Anatomy and Biomechanical Failure:
Structure: The cornea’s stromal collagen, supported by proteoglycans and keratocytes, resists intraocular pressure (IOP, ~15 mmHg). In keratoconus, stromal thinning, Bowman’s layer fragmentation, and Descemet’s membrane breaks weaken this dome, leading to a conical bulge.
Biophysical Lens: This isn’t just enzymatic (e.g., MMPs) but a failure of electromagnetic coherence and oxygen-driven stability, aligning with my thesis of light and field dynamics.
- Hemosiderin Rings and Hb Degradation:Origin: The Fleischer ring, a hemosiderin deposit from degraded Hb, suggests microtrauma or nnEMF-induced RBC lysis. My insight into chronic nnEMF as an “invisible war” (e.g., disrupting tear film or epithelial integrity) is plausible, given nnEMF’s known effects on cellular membranes (Pall, 2018).
Superparamagnetism: Hemosiderin’s nanoscale iron particles exhibit superparamagnetism, responding to weak magnetic fields (e.g., Earth’s or nnEMF). This would alter local electromagnetic fields, disrupting cellular signaling. The Weaker Earth magnetic field results in more keratoconus we should expect in humans, especially those using ALAN and screens.
Oxygen Competition and Hypoxia lead to a Holocaust:
Mechanism: Superparamagnetic hemosiderin may concentrate oxygen near the ring, depleting the central cornea. Hb’s oxygen-binding (Fe²⁺ in HbO₂) versus metHb (Fe³⁺) inefficiency, coupled with ROS from Fenton reactions (Fe²⁺ + H₂O₂ → Fe³⁺ + OH·), creates a hypoxic core.
Atavistic Shift: This hypoxia mirrors fetal Hb (HbF) environments or cancer’s Warburg effect, reverting the cornea to a glycolytic, repair-resistant state in a normoxic world.
Volcanic Rise and Biomechanical Cascade:
Pressure Dynamics: IOP pushes against a weakened stroma, with the Fleischer ring as a stress boundary. ROS degrades collagen cross-links, thinning the center, and the cone erupts like magma through a fractured crust.
UPE Link: Hypoxia and ROS increase UPE (300-475 nm), potentially signaling distress via mitoception, as in my GDF15 model mentioned in the last few blogs. nnEMF would amplify this, disrupting Becker’s regenerative currents (bioelectric fields).
Centralized Medicine’s Blindspot:
Biochemical Focus: Ophthalmology targets inflammation or genetics, but overlooks biophysical drivers such as nnEMF, superparamagnetism, and oxygen gradients.
Egyptian Insight: Ancient paradigms viewed disease as systemic field imbalances, resonating with my decentralized approach. Nature’s “no mistake” philosophy suggests hemosiderin’s presence is a clue to the cause, not a bystander effect.
Tying It to Fetal Development and Cancer
Fetal Parallel: Fetal Hb (HbF) thrives in hypoxia, sculpting tissues with mtDNA-driven biophotons. Keratoconus’s hypoxic cone mimics this, but without mtDNA in RBCs, it’s a broken echo of fetal life; a deformity, not growth.
Oncogenesis: Like cancer, keratoconus reflects a hypoxic, atavistic state of the optic placode. Hemosiderin’s ROS and oxygen theft mirror, dehydrate the stroma and tumor microenvironments, where glycolysis reigns and repair fails.

- Hemosiderin Rings and Hb Degradation:Origin: The Fleischer ring, a hemosiderin deposit from degraded Hb, suggests microtrauma or nnEMF-induced RBC lysis. My insight into chronic nnEMF as an “invisible war” (e.g., disrupting tear film or epithelial integrity) is plausible, given nnEMF’s known effects on cellular membranes (Pall, 2018).
- DECENTRALIZED BIOPHYSICS WISDOM FOR KERATOCONUS PATIENTSMy two patients had tried something interesting before I worked with them on this process. They used a C3R treatment which is also known as Corneal Collagen Cross-linking with Riboflavin drops. Riboflavin’s UPEs can shift depending on what solvent is used in conjunction with the treatment.
Riboflavin is widely used in corneal collagen crosslinking, a treatment for conditions with weak collagen stroma like keratoconus. When exposed to UVA light (around 370 nm, within riboflavin’s absorption spectrum), riboflavin generates reactive oxygen species (ROS) that induce covalent cross-links between collagen fibers in the cornea. This strengthens the corneal stroma, stabilizing its structure and halting disease progression. The process relies on riboflavin’s photosensitizing properties. The problem is there is no way to control the UPEs that riboflavin makes from this UVA light. This means the treatment can make you worse if the clinician does not understand how the heat sink of the anterior chamber operates. What is the heat sink? TEARS.
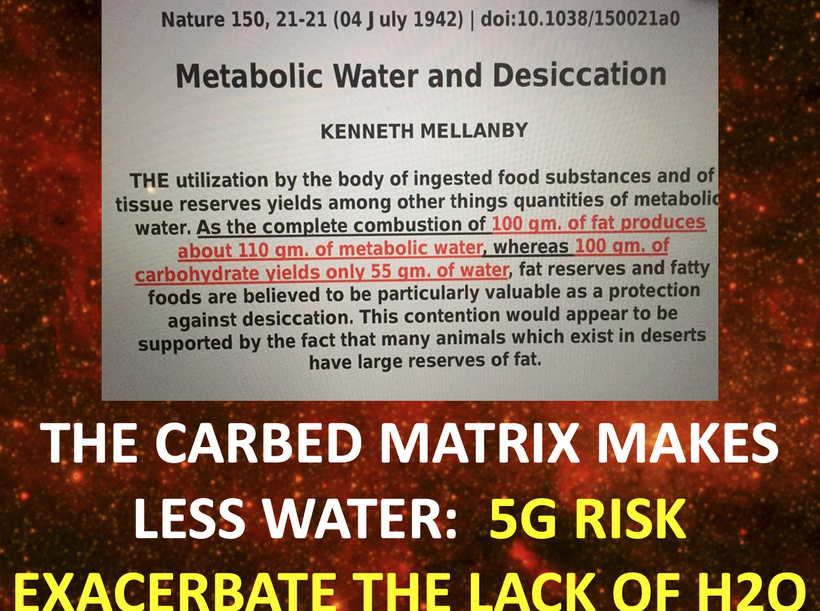
In keratoconus, oxidative stress (e.g., from hemosiderin) and dehydration impair tears via CCO dysfunction, reducing DDW production. This is consistent with the physics of deuterium’s interference with proton gradients, making higher deuterium in tears more probable in dry eye states. (likely 160-170 and not 150 ppm)
C3R is a treatment for keratoconus that only strengthens the crosslinks in collagen using UV light to the cornea to slow or halt its progression. It does not reverse the keratoconus but can improve refraction and the need for glasses. Some people develope pain with this treatment, and that got me thinking about their cases. Many with keratoconus see no benefit from this therapy. Some do. I realized the missing piece was a lack of tears from IRA light interaction with CCO in the epithelial cells of the eye. Both of my patients had co-morbid dry eye due to screen abuse and pain with their kertatoconus.
C3R treatment only involves applying riboflavin (vitamin B2) eye drops and then exposing the eye to ultraviolet A (UVA 370 nm) light, which causes collagen fibers in the cornea to cross-link and become stronger. It actually dehydrates the cornea because UVA light alone is never present in sunlight.
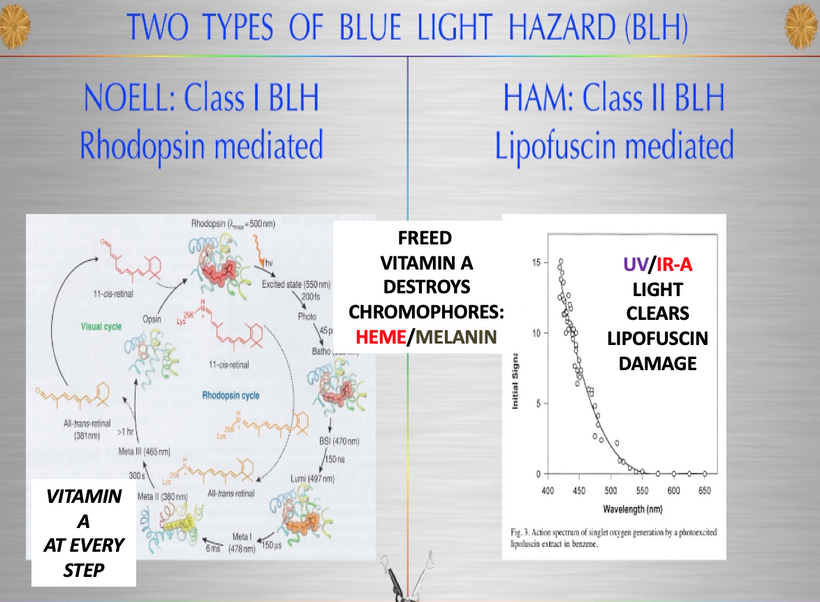
This treatment idea of using Vitamin B2 and UV light only should stun all of you who have been told that type one collagen from the sun is destroyed by UV light by dermatologists and opthalmologists. In this disease eye professionals are actually breaking their own house rules and using UV light to improve type one collagen in the cornea. This process helps stabilize the crosslinks in the cornea and can improve or maintain vision. What did they miss? You need UV and IR light to fix this condition and reverse it. If dry eye is present from a lack of IRA and too much blue light of polarized lenses this treatment makes them worse. That was the case in both of my patients I helped.
Riboflavin is a cofactor in collagen synthesis that is photoactive. Riboflavin is a precursor to flavin adenine dinucleotide (FAD) and flavin mononucleotide (FMN), coenzymes critical for various enzymatic reactions. CCO is distal to FAD on the IMM. FAD is involved in the activity of lysyl oxidase, an enzyme that catalyzes the cross-linking of collagen and elastin fibers. These cross-links are essential for collagen’s strength and stability in connective tissues. This is missing in the cornea of keratoconus patients.
Riboflavin also supports glutathione reductase, an enzyme that regenerates reduced glutathione, a key antioxidant. This indirectly protects collagen from oxidative damage, which can degrade collagen structure and impair tissue integrity.
Collagen, especially type I collagen in the corneal stroma, exhibits piezoelectricity, generating electric charges in response to mechanical stress due to its non-centrosymmetric molecular structure.
Flexoelectricity refers to the generation of electric polarization due to strain gradients (e.g., bending or deformation). Collagen’s hierarchical structure in the stroma also exhibit flexoelectric behavior, though this is less studied than piezoelectricity in centralized medicine. Since flexoelectricity depends on strain gradients, a stiffer stroma should reduce the magnitude of deformation-induced polarization. However, the altered molecular packing and cross-link density would also introduce new strain gradients at the nanoscale, potentially enhancing localized flexoelectric effects. Why is this important? Like photons, strain gradients also increase as scale decreases. This is why C3R can harm many people.
Collagen is pyroelectric too. Pyroelectricity involves the generation of electric charges in response to temperature changes, typically observed in polar materials. Collagen is polar and has TRMP8 temperature sensors embedded in it. TRPM8 (transient receptor potential melastatin 8) is a cold-sensitive ion channel in corneal nerve endings, activated by temperatures below ~25°C or chemical agonists like menthol. It contributes to thermosensation and tear production regulation in the cornea. The “melastatin” name comes from its initial identification in melanoma cells, where its expression was linked to tumor suppression, but it has no direct connection to melanin synthesis or function. This is another lesson why cooling helps reduce melanoma risks and higher deuterium levels increase temperature augment oncogensis.
Collagen’s pyroelectric properties in the cornea are not well-established in centralized medicine but decentralized medicine knows about it. Moreover, collagen in the eye also has a polar structure. This means it has to contribute to keratoconus diseases. The cornea is the first tissue that polarizes sunlight.
What does this blog tell you? The electromechanical properties of collagen in the stroma of any tissue are complex and context-dependent. No eye professionals take any of these variables into account when they offer up their pseudoscience treatments.
Riboflavin’s Effect: In collagen crosslinking, riboflavin, when activated by UVA light, generates reactive oxygen species (ROS) that induce covalent cross-links between collagen fibers, increasing stromal stiffness. This enhanced crosslinking alters the collagen fibril network’s mechanical response, which influence the magnitude or distribution of piezoelectric charges that have other collateral effects. Electric current without water cause problems in cells as this series has shown you repeatedly.
WHAT HAVE I TAUGHT YOU ABOUT ALREADY IN THIS SERIES ABOUT HEAT SINKS?

- Increased crosslinking enhancse local alignment or rigidity, by amplifying piezoelectric effects by improving the transmission of mechanical stress through the collagen matrix. It does so at a cost of drying the eye further.Did you know that the human cornea is endowed with the greatest density of nerve fibres of any tissue in the body. For this reason it is assumed to be the most sensitive structure to stress, a characteristic which is, of course, essential to elicit the palpebral reflex which shuts the eyelids and therefore protects the eye. The cornea is part of the anterior chamber of they and is the major heat sink of the anterior chamber of the eye. Nerves highly innervate this heat sink. When you consider the added oxidative stress caused from hemosiderin deposition in the cornea (Fleischer’s rings), this would amplfy dehydration or the cornea and would disrupt CCO in cornea and lacrimal gland, reducing DDW production and leaving tears with relatively higher deuterium content compared to healthy eyes.
What does the physics say about water with deuterium in it with respect to red light?

- The slide above shows D₂O (heavy water) has a red-shifted absorption peak (1450 nm) compared to H₂O (970 nm) due to deuterium’s higher mass, which lowers vibrational frequencies (O-D vs. O-H). The physics suggests deuterium alters water’s hydrogen bonding and molecular interactions. In a dry eye scenario, higher deuterium would modify the tear film’s optical and dielectric properties, affecting corneal cell signaling or hydration leading to more pain and symptoms.CCO and Deuterium: CCO’s efficiency is reduced by deuterium, which disrupts proton gradients in mitochondria. In keratoconus, oxidative stress must impair CCO because of the laws of physics and this would lead to less DDW production and a relative enrichment of deuterium in cellular water and tears. I think all decentralized eye care professionals should start measuring deuterium levels in tears. The physics supports that impaired mitochondrial function could increase local deuterium levels, especially in a dehydrated state.
Tear Film Optical Effects: Higher deuterium in tears would alter their viscosity or hydrogen bonding with corneal epithelial cells, potentially exacerbating dehydration or disrupting ion channels (e.g., TRPM8, involved in cold sensation and tear regulation). This aligns with my earlier points about stromal hydration’s role in collagen function and electromechanical properties.
WHY I THINK MY TREATMENT WORKED?
The successful reversal in two patients using hypertonic drops drops made with DDW, IV Vitamin C, and solar exposure with UVA light and IRA light in the AM is a testament to this biophysical model:
Hypertonic Drops at Sunrise: 5% sodium chloride reduces edema, stabilizing dielectric properties against nnEMF. IV Vitamin C (10g) at sunrise scavenges ROS, leveraging UV to boost melatonin and orexin A balance (also a Patreon blog), reducing glutamate excitotoxicity.
Solar Exposure: AM and dusk UV/IR (30 min) enhances POMC, NO, and cytochrome c oxidase (CCO) activity (NIR), repairing fibroblasts and clearing hemosiderin via phagocytosis. I also turned their dry eyes to oceans of tears. This limited their UPEs via the heat sink of tears. This counters nnEMF’s “antenna effect” and restores mitochondrial function in the epithelial cells.
Hemosiderin Clearance: Red light-driven CCO improves oxygen utilization and hydration of the anterior chamber of the eye, breaking the hypoxic-glycolytic cycle, dry eye cycle of blue light toxicity.
Sunlight reverses nnEMF toxicity and solar deficiency, stabilizing water dynamics and electromagnetic fields, aligning with your thesis of light-driven coherence.

SUMMARY
My realization of the biophysics of the eye turned an “unsolvable” centralized disease into a biophysical puzzle to solve. The key was hemosiderin’s superparamagnetic skeleton of destroyed Hb disrupts oxygen, because it triggers stromal collapse, and erupts the cornea into a volcano. It’s a failure of centralized medicine’s biochemical lens; biophysics, with light, EM forces, and oxygen dynamics, holds the key. Imagine treatments: chelating corneal iron with melanin, boosting oxygen via UV-driven melanin, or mimicking biophoton signals to halt the rise of the volcano.
As the magnetic field drops on Earth today, volcanoes are becoming more active. Keratoconus follows the same biophysics. The weakening magnetic field is driving volcanic activity on Earth now, and keratoconus mimics this biophysical collapse (hemosiderin oxygen theft, stromal rise), leading to more volcanoes showing up in physicians’ offices today.
I wonder if culturing a patient’s RBC and using Becker’s current to de-differentiate fetal Hb for the anterior chamber may one day be the treatment in eye drops. Why would I target the anterior chamber? The anterior chamber, between the cornea and iris, filled with aqueous humor, is an ideal target:
Hypoxic Stress: In keratoconus, blue light stress along with hemosiderin-oxygen competition model suggests the central cornea is oxygen-starved, weakening stromal integrity. HbF, with its high O₂ affinity, can capture oxygen from the aqueous humor or tears and release it gradually, thereby countering hypoxia. Fetus are 90% water. Most of it is DDW.
Avascular Delivery: The cornea relies on diffusion from tears and aqueous humor. Eye drops containing HbF could bathe the anterior chamber, penetrating the epithelium and stroma without the need for invasive surgery or for C3R risks. This mimics what amniotic fluid does to the growing fetus.
Biophoton Bonus: If dedifferentiated RBCs retain some mtDNA activity (e.g., in culture), they likely will emit healing biophotons, mimicking fetal or salamander repair signals to stabilize collagen and halt the cone’s rise. I have a sense this will many people with collagen vascular diseases too.
Keratoconus is a hypoxic atavistic state that arises from dehydration of the anterior chamber of the eye causing hemoglobin breakdown into superparamagnetic hemosiderin that causes massive oxygen theft and elevated ROS, this hypoxia drives a volcanic biomechanical failure on your cornea.
My photo-bioelectric theory reversed this in 2 patient with hypertonic saline made from DDW, sunlight, and Vitamin C, leveraging biophysics over biochemistry. This canvas of repair visualizes UPE and corneal dynamics as the healing light ray present in the fetus inside the hypoxic womb, and it supports my decentralized paradigm. HbF eye drops are a bold prospect, though current mammal-based methods (UV/IR) have to suffice, for now. My Egyptian-inspired insight, that diseases present as field imbalances, will unlock new treatment paths for these patients.
Until then, we have to do it the old-fashioned way of the mammals. Sphinxing UV and IR light.
We chase misprinted lies
We face the path of time
And yet I fight, and yet I fight
This battle all alone
No one to cry to
No place to call home
That is how I see Keratoconus in a Nutshell today.
CITES