This video blog is designed to show that Thomas Paine and Nayib Bukele have much in common.
Politically they are doing the same things to their countrymen.
Thomas Paine was born on February 9, 1737, and died on June 8, 1809. He was an English-born American political activist, philosopher, political theorist, and revolutionary. He authored Common Sense (1776) and The American Crisis (1776–1783), two of the most influential pamphlets at the start of the American Revolution, and helped inspire the Patriots in the 13 colonies of New America in 1775 to declare independence from Great Britain. He wrote Common Sense at the age of 38. On September 7th, 2021 Nayib Bukele was 38 years old when he made Bitcoin legal tender in El Salvador. Both of these men were Millenials of their day. Paine’s ideas reflected the Enlightenment-era ideals of transnational human rights. Bukele’s political ideas have changed to support the same ideology. Paine convinced poor farmers who sought refuge from King George over religious freedom and freedom from unjust taxation. Bukele is doing the same by giving his poor country monetary freedom to fight the lender of last resort known as the IMF. The IMF represents the same ideology as King George.
What Paine said in “Common Sense” describes Bitcoin perfectly for mankind in 2022.
Paine wrote, “Perhaps the sentiments contained in the following pages, are not yet sufficiently fashionable to procure them general favor; a long habit of not thinking a thing wrong, gives it a superficial appearance of being right and raises at first a formidable outcry in defense of custom. But the tumult soon subsides. Time makes more converts than reason.
As a long and violent abuse of power, is generally the Means of calling the right of it in question (and in matters too which might never have been thought of, had not the Sufferers been aggravated into the inquiry) and as the King of England had undertaken in his own Right, to support the Parliament in what he calls Theirs, and as the good people of this country are grievously oppressed by the combination, they have an undoubted privilege to inquire into the pretensions of both, and equally to reject the usurpation of either.
In the following sheets, the author hath studiously avoided everything which is personal among ourselves. Compliments, as well as censure to individuals, make no part thereof. The wise, and the worthy, need not the triumph of a pamphlet; and those whose sentiments are injudicious, or unfriendly, will cease of themselves unless too many pains are bestowed upon their conversion.
The cause of America is in a great measure the cause of all mankind. Many circumstances hath, and will arise, which are not local, but universal, and through which the principles of all Lovers of Mankind are affected, and in the event of which, their Affections are interested. The laying of a Country desolate with Fire and Sword, declaring War against the natural rights of all Mankind, and extirpating the Defenders thereof from the Face of the Earth, is the Concern of every Man to whom Nature hath given the Power of feeling; of which class, regardless of Party Censures, is the
THE AUTHOR.
Philadelphia, Feb. 14, 1776.”
On June 5, 2021, El Salvador President Nayib Bukele declared that bitcoin, the first cryptocurrency, would become legal tender in El Salvador. A few days later, the Bitcoin Law was passed, to take effect on Sept. 7, 2021.
Bitcoin restores and provides monetary freedom to the people. This is the only freedom that was not spoken about by Thomas Jefferson in the Declaration of Independence of July 4th, 1776. The reason should be obvious: the idea of Bitcoin was 233 years away from 1776. Ironically, the corrupted democratic republic would fund and build the internet that would act like John the Baptist for the introduction of Bitcoin by Satoshi Nakamoto. Bukele seemed to realize that monetary freedom would be the seed to sow if he wanted to rid his country of poverty and the slavery of IMF debt. Most of his population however has no idea how this idea works. Moreover, his political allies want the public to believe that Bitcoin is Bukele’s coin or his idea. It is far from the truth.
What Bukele gave his people on Sept 7th, 2021 was a new Declaration of Independence from IMF rule. September 7th, 2021 was an action that mimics precisely what Paine wrote above in words. He gave them a reason to fight for freedom. Freedom comes in a negative and positive forms. One is “Don’t Tread On Me” (negative), and the other is “We The People” (positive). Patriots of the 13 colonies had to fight for their freedom and liberty in a revolutionary war. The people of El Salvador, today, really have no idea what Bitcoin is or who Paine was and what he did for future Americans, but they do not have to wage war against their King today. That King is the IMF, their current debt holder. They just need to buy Bitcoin to fight their King and push him to submission. People who are forced to use paper money are going to have to fight the peaceful quiet riot until we have to wage the real war against the banking elites.

Bitcoin is more than just a wise investment of the present day. It’s poised to become the central player in the future of money itself. Money, which has evolved through the millennia from cowrie shells to clay tablets to precious metals, banknotes, and bank balances, is taking another step into the future. Money is becoming digital. Governments linked to the IMF and BIS want to create centralized digital money called SDRs or CBDCs. All of these technologies limit the freedom of people using them in a myriad of ways. This suits the government but it does nothing for the things written in the Declaration of Independence or the US Constitution.
Thomas Jefferson’s words in our Declaration of July 4th, 1776 rhyme quite well with the actions of Nayib Bukele on Sept 7th, 2021.
Jefferson wrote, In Congress, on July 4, 1776,
“The unanimous Declaration of the thirteen united States of America, When in the Course of human events, it becomes necessary for one people to dissolve the political bands which have connected them with another, and to assume among the powers of the earth, the separate and equal station to which the Laws of Nature and of Nature’s God entitle them, a decent respect to the opinions of mankind requires that they should declare the causes which impel them to the separation.
We hold these truths to be self-evident, that all men are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty, and the pursuit of Happiness.–That to secure these rights, Governments are instituted among Men, deriving their just powers from the consent of the governed, –That whenever any Form of Government becomes destructive of these ends, it is the Right of the People to alter or to abolish it, and to institute new Government, laying its foundation on such principles and organizing its powers in such form, as to them shall seem most likely to effect their Safety and Happiness. Prudence, indeed, will dictate that Governments long established should not be changed for light and transient causes; and accordingly, all experience hath shewn, that mankind are more disposed to suffer, while evils are sufferable than to right themselves by abolishing the forms to which they are accustomed. But when a long train of abuses and usurpations, pursuing invariably the same Object evinces a design to reduce them under absolute Despotism, it is their right, it is their duty, to throw off such Government, and to provide new Guards for their future security.–Such has been the patient sufferance of these Colonies; and such is now the necessity which constrains them to alter their former Systems of Government. The history of the present King of Great Britain is a history of repeated injuries and usurpations, all having in direct object the establishment of an absolute Tyranny over these States. To prove this, let Facts be submitted to a candid world.” Jefferson then went on to state the case of facts at that present moment of why freedom from the King’s tyranny was wise for New America. History has documented this movement 246 years ago.
13 years ago Bitcoin was born. Bitcoin is the “musket rifle” that Bukele has chosen to use against the IMF for the benefit of his people.
Governments have become quite eager to defend the status quo where states and state-based institutions have a monopoly on money printing, and corporations also have their sights set on the reinvention of money. In this regard, Bukele sticks out like a sore thumb to most other politicians in the world. He wants to return the freedom of money back to his people for them to decide how to live their life. But there are a number of factors that over time will work in Bitcoin’s favor.
First, Bitcoin is censorship-resistant and offers freedom from financial repression.
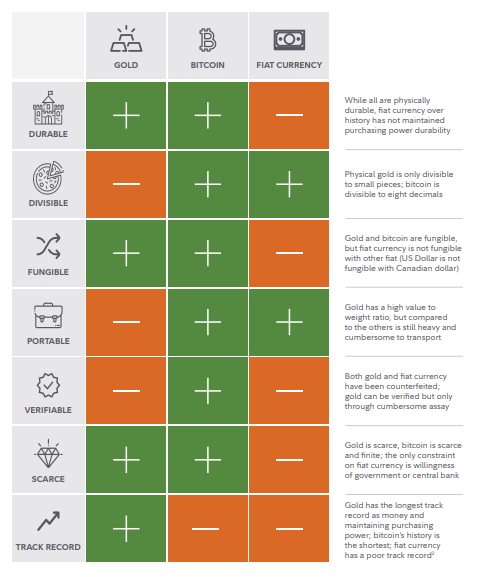
- Second, Bitcoin is emerging as the natural successor to gold as a store of value over time.
- Third And somewhat counterintuitively, Bitcoin is benefiting from the efforts of legacy financial technology and payments companies like Western Union, PayPal, Block, and Visa that are making Bitcoin available to their hundreds of millions of users and millions of merchants.
- Fourth, Bitcoin is being embraced by large public companies and other institutions as a viable alternative to cash and other assets on their balance sheets or in their portfolios.
- Fifth, Bitcoin’s community is borderline religious in their devotion, which makes Bitcoin resilient in the USA. This freedom fever is spreading to communities in El Salvador and Central and South America as it did in the 13 colonies during Paine’s lifetime.
Bitcoin is censorship-resistant which creates freedom emergently. In other words, a government cannot throttle, control or monitor your behavior as they can in the legacy financial world. Consider the following examples from Nigeria, Canada, India, Belarus, China, and Russia, collectively home to 3 billion people.
In 2020, protests against the government erupted in Lagos and across Nigeria because of the brutal and illegal actions of a unit in the police force called the Special Anti-Robbery Squad (SARS). Within days, groups supporting the protesters had their bank accounts frozen. With no other option, they turned to Bitcoin, raising funds that sustained the movement. We saw the same thing in Canada in the winter of 2022 in Canada, when the Truckers began to use Bitcoin to throttle the tyranny of Trudeau.
In Nigeria, daily U.S. dollar peer-to-peer trade consistently clocks in at over $1.5 million USD from a base of zero only a few years ago. Peer-to-peer Bitcoin transactions can be zero-fee, a big break from the much higher fees many in Africa are forced to pay for basic financial services, such as those for remittances which average 9%. You saw the video above when Salvadorean told us he gave up 30% of his salary to send his money home to Salvador using Western Union.
Nigeria’s young, tech-savvy Bitcoin users are the model for how the global south in Central and South America will soon interact with financial services. In China, the government wants to replace many transactions with a central bank digital alternative to control the behavior of how people use money to buy things. In India, the government too high denomination notes out of the circulation to limit counterfeiting.
The demise of cash highlights the need for a digital alternative to ensure private, safe payments between individuals. For example, in China without cash, your access to credit, payments, and savings can simply be switched off if you disagree with the government, a form of financial deplatforming. We have experienced deplatforming in the US on social media if you have a different opinion from the paradigm in power. This idea is all around us now and is a detriment to our inalienable rights to freedom. Bitcoin is a prescription to this illness.
Bitcoin promotes freedom. It enables anyone, anywhere to send, receive or store their wealth. It also prevents governments or corporations from meddling in these transactions. But what type of freedom does Bitcoin provide? Is it a freedom to use or store digital cash or the freedom from an overreaching state? This shows the world why Bukele is no dictator. HE is giving his people something tangible they can use to protect them from the government long after he is gone. This is precisely what the purpose of the founding documents of the USA was about. Thomas Paine’s pamphlets set the stage for these documents. Those pamphlet’s changed public opinion in the 13 colonies about freedom and its costs. I have a sense that Bitcoin’s change to legal tender status in El Salvador will soon do the same for Salvadoreans. I think we can see this when we look at the megaphone that resides in El Zonte at the Hope House.

13 years ago, the project called “Filling the Love Tank of El Zonte´s Children ” a project created by Jorge Valenzuela and his wife Cristina Guillen by the mentoring of Michael Peterson and his wife Britney Peterson who brought their philosophy of life to Jorge and Cristina. From this idea came a community that supported a new open-loop community that embraced the use of Bitcoin in a peer-to-peer fashion. This idea grew so spread monetary freedom to the poorest in El Salvador. They now go all over El Salvador to show other communities how to use Bitcoin and better themselves and embrace freedom.
FREEDOM IS MORE COMPLICATED THAN IT APPEARS
Freedom in the republican sense is a social consensus, as the distinction between a master and a slave. Under such a system, interference does not have to be exercised – the master does not have to crack his whip – for it to be present: The mere existence of external, obtrusive forces makes one unfree.
Liberal freedom, on the other hand, is the condition of being free as long as a master does not interfere arbitrarily. ‘Don’t tread on me’, is the cliche that represents this idea.
Bitcoin is based not on the idea of liberal freedom, but on republican freedom. This is not Bukele’s idea. Bukele is borrowing this idea from Paine and Jefferson who borrowed it from ancient Rome. The American Revolution against British domination was a positive conception of freedom = “We The People” in the Constitution of the USA. It is best described as the ability to dosomething with the aim of realizing a goal or more fully reaching one’s potential.
The positive conception of freedom is a negative concept because it is based on the absence of something, in this case, domination, and a positive one because it relies on active citizenship. For this reason, it offers a more comprehensive approach to freedom, especially with respect to how government and politics operate.
From this wellspring, Bukele borrowed this version of freedom from Paine and Jefferson because it’s this type of freedom that Bitcoin makes space for in El Salvador today because the democratic process facilitates choice. It’s about self-mastery. This makes Bukele share some traits with Paine and Jefferson. It also means Bukele respects what happened in ancient Rome.
Bitcoin, as the only decentralized blockchain technology, not only has the advantage of being free from outside interference but also implements various mechanisms agreed upon by its governance protocols to secure that freedom. This is how Bitcoin creates self-mastery in its code. Any “interference” to Bitcoin’s protocol has to be deliberated on, and consented to, by the core developers and node operators before it is approved and implemented. This is very similar to the US Constitution. For example, amending the U.S. Constitution requires a two-thirds majority vote in both the House of Representatives and the Senate. Then it must be ratified by three-fourths of the legislatures in the 50 states. If the degree of consensus across a wide body of people is a measure of success, then we can see why Bitcoin uses a proof of work consensus to provide for the freedoms of its users.
What Bukele’s political opponents fail to realize is that the Bitcoin blockchain protocol promises both negative freedoms (“Don’t Tread on Me”) and positive freedom (“We the People”) it attracts not only libertarians but also progressives. This means Bitcoin will eventually attract ideologues in both Arena and FMLN to his Bitcoin policies. Neither of these two factions of political ideologues realizes that Bukele is stealing their political power right below their noses.
Today, the right and left in the USA do not argue about the truths in the Declaration of Independence or the Constitution. They both support it. In the future, Arena and FMLN will come to the same conclusion about Bitcoin.
The US Constitution and Declaration were missing the major part of freedom, namely, the freedom of money. Bitcoin solves this problem. El Salvador has solved the toughest problem. The key is when will the old world political parties realize that Bukele has used the playbook of Thomas Paine and Jefferson to solve the problem that has plagued El Salvador for decades?
It seems his people trust him now, just like the original 13 colonies trusted George Washington not to become a new version of King George under the guidance of our Constitution which provided governance of the newly born USA. These words are synonymous with the code found in Bitcoin today.
CITES
Mankind’s collective ideas on freedom.