Many forget light is both a particle and wave. It has a duality. Life uses that advantage. Light from the sun acts more like a wave than a particle and that is how we use it as ainformation. Light created by photosynthesis (food) or by cells (bio-photons) acts more like a particle. No one should forget both pathways LIGHT IS INFORMATION. How it is used as information is what varies in Nature. I covered that here.
INTRODUCTION
Do you use time wisely? Do you prioritize your choices by weighing the value of information and wisdom against the cost of choice and decision?
Life always is wrapped in opportunity cost.
Decentralized medicine is both science and art in a unique package blended by perspectives of how the world is affected by Nature. Looked at from this vantage point, a good decentralized artist knows he has less time than ideas and this pushes him to act, to create, and to share his ideas born in his craft. Time is too precious to waste.
The job of the Nature is to always deepen the mystery for the artist. The job of the artist is to find the inspiration of Nature and reflect it in your creation and wisdom.
Optical biophysics studies how light is transformed into information for cells. Cells are filled with non-visual photoreceptors to capture the electromagnetic properties buried in photons of the cosmos. Biology is not a foundational science. Physics is. Optics forms the solid-state physics of the living state. This means paying attention to the light emissions and absorption frequencies from cells, DNA, and molecules of organic matter and how these interface with water. At birth, we are 80% water; at age 60, we are at 55-60% water by weight. Cells capture light and create water and are moderated by the nested array of electric and magnetic fields transformed by mitochondria located on the quantum level and capable of stretching up to the galactic level where plasma is ubiquitous. This plasma connects everything in an electrical circuit at unfathomable ranges and power. We do not operate at all ranges of this spectrum. This plasma has a pulse or rhythm to it. Our cells pay attention to this music and to its rhythm. The rhythm can be found in the absorbtion and emission spectra of a molecule.
Melatonin is a hormone that is naturally made by the mitochondria in your tissues, and its production is closely tied to light. In response to darkness, the mitochondria in our tissues initiates production of melatonin but light exposure at might or artificial light during the day slows or halts that production in mitochondria. The pineal gland is not where the melatonin story begins on circadian clock maintence.
This is the range of nature’s music, which we are part of and can tune into. All parts of this spectrum have biological effects. Some are good, and some are harmful to cells. This is the nature of light exogenous to our cells.
The organism creates its own music endogenously— of a somewhat more restricted but still enormous range between 10^-7 m and 10^8 and beyond — it is both exquisite and subtle. With the present level of ‘man-made’ electromagnetic pollution of the environment, one might very well ask whether the organism’s melody is in grave danger of being drowned out altogether by our mitochondria.
When we listen to a good talk, book, or podcast, whether off-the-cuff or seared into our memory by emotion, something in us is built to hear this music, not just in its register, the lilt, the cadence or its rhythm, but, in those moments, there are no words to be heard; all you can hear is the enveloping silence.
The same is true with cells…..the photons in the sun are sounds, while the silence is found in the darkness of night. The real music of life is found at night when light is absent. This is why ALAN, called artificial light at night, is so dangerous to humans. Feedback coupling has many facades in reality, and few in centralized science realize it.
Melatonin is made in the morning and during the day, but it only acts to delocalize electrons under the cover of darkness. Melatonin is like a conductor of Nature’s music. Few understand how sunlight gives its information to serotonin to create melatonin in our mitochondria. Sunlight transforms serotonin into melatonin and melatonin, then IMBIBES our cells with quantum information to ensure cells display significantly higher amounts of both p53 and acetylated p53. This biochemical signal is the basis of the anticancer effect of mitochondrial melatonin. This is how light becomes biochemical information.
Not to discount the bio-chemical nature of life, which is hegemonic in the health science realm, the optical bio-physician asks: which of these is PRIMARY in the growth, replication, and division of labor of individual cells or entire species of organisms? Is it the chemical attributes of living matter or the electromagnetic properties?
Mitochondria, the transformer of light to melatonin, are not mechanical machines; you should never think of them this way.
Mechanical systems work by centralized control. Centralization is a hierarchy of controllers and the control that returns the systems to set points (equilibrium). Life is never at equilibrium. Mitochondria are fully built to be decentralized to light and dark cycles.
HOW DID WE COME TO KNOW THAT LIGHT IS INFORMATION AND BOTH LINK TO ENERGY?
Claude Shannon is regarded as the father of information theory. Alan Turing is known as the father of computer science. In 1943, Shannon and Turing worked on different projects at Bell Labs in New York City.
In 1948, intersecting with Shannon’s pioneering theory on information, Alan Turing simultaneously wrote a report at the National Physical Laboratory on “Intelligent Machinery” that laid the groundwork for the emerging fields of information networks and artificial intelligence.
They had discussions together, including about Turing’s “Universal Machine,” a type of computational brain. Turing seemed quite surprised that in a sea of code and computers, Shannon envisioned the emergence of arts and culture as an integral part of the digital revolution – a digital mitochondria of sorts. What was dreamlike to Turing’s imagination in 1943 has become today’s reality. Shannon’s early connections between the arts, information, entropy, and computing intuit the future we are experiencing today. Turing famously said “Shannon wants to not just feed data to a brain, but cultural things! He wants to play music to it!” Shannon knew there was art buried in the nature of information. There was an inherent rhythm in both men’s ideas.
Order and chaos are deeply linked in nature by rhythms. The paper above was the first paper that showed us how feedback loops could organize chaos in light & dark to build circadian biology using waves in rhythm. It requires no complexity and is a feature of Nature’s self-organization ability. All it requires is a feedback loop to operate. Turing was the first to crack the key biological rhythms in life.
WHAT DID TURING STUMBLE INTO?
More light = more information in the system to build complexity. Darkness makes the information durable and usable. Energy tends to dissipate in the universe — and entropy, a measure of its dissipation, increases over time.
Time appears as entropy in cells and is coded for by molecular clocks. All clocks are flow meters of entropy. This is how matter organizes disorder into order. When a dissipative system controls entropy, life can manifest. This is a very basic idea in quantum biology that Turning explored before quantum biology became a disciple of decentralized science.
Three years before Turing’s paper in 1951, Claude Shannon shook up the world with his work on information theory.
In 1948, Claude Shannon’s paper showed that entropy is linked to information. Entropy is a way to measure the amount of information in a source. The more information you have, the higher the entropy of the source is. A high-entropy message means low information gain and a low-entropy message means high information gain. Biology wants to create a low entropy game in cells so cells can collect massive amounts of information. Mother Nature built cells filled with clocks to take advantage of this idea. Information gain can be thought of as the message fidelity in a system: the amount of clean knowledge available in a system.
To physicists John Wheeler, the ideas of Turing and Shannon implied energy and information are deeply linked. John Wheeler proved that was true in physics using the Landauer Principle (1961). Biologists still have no idea about the implications of this work.
Landauer’s principle is a physical principle pertaining to the lower theoretical limit of energy consumption of computation. It holds that an irreversible change in information stored in a computer, such as merging two computational paths, dissipates a minimum amount of heat to its surroundings. Landauer’s principle states that the minimum energy needed to erase one bit of information is proportional to the temperature at which the system is operating.
At room temperature, the Landauer limit represents an energy of approximately 0.018 eV (2.9×10^−21 J). Modern computers in 2023 use about a billion times as much energy per operation. This means information transfer in nature always has an energy cost. This is why nature uses a PoW mechanism. It explains why John Wheeler said information and energy are the same physical entity in Nature. It might also explain why cells are filled with water to dissipate the effect of heat created during information processing. Remember water has a massive heat capacity.
Wheeler divided his own life into three parts. The first part he called “Everything is Particles.” The second part was “Everything is Fields.” And the third part, which Wheeler considered the bedrock of his physical theory, he called “Everything is Information.”
When Shannon was at Bell Lab in 1948, Bell labs had tons of information buried in their messages but had no way to mine or collect the information to make the data useful. Shannon thought about the problem and wrote a paper about using mathematics to data-mine information.
The paper was called “A Mathematical Theory of Communication.”
Once Shannon connected these dots mathematically, it opened the door to signal processing, compression, and converting messages into an algorithm code to transmit them digitally. It gave rise to the Cambrian revolution in computers after 1948. Turing died in 1951, but his ideas lived on in many computer engineers.
THE LINK TO ENERGY AND THERMODYNAMICS
Shannon’s limit in information transfer mathematically looks exactly like Boltzmann’s equation for entropy in thermodynamics. Entropy was an idea originated in the 1824 by Carnot. I’ve written Patreon entries on Carnot’s theorem. Both concepts, bit and photon, share the same roots: nineteenth-century thermodynamics and the concept of entropy.
In 1877, Boltzman gave us a statistical explanation of the second law of thermodynamics. In 1877, he provided the current definition of entropy. Shannon’s papers gave us a similar answer for information as his equation shows below.
Because these two equations are nearly identical mathematically, physicists began to realize in the 1960s that information and energy are linked physically in reality. Nature is revealing her secrets in these equations.
Shannon’s work on information entropy links to Michael Crawford’s theory on DHA. These ideas coordinate with Einstein’s special relativity (1905). Einstein’s work directly ties to the Landauer Principle (1961) to explain how cells use light to communicate. Information transfer costs us energy.
Landauer predicted that erasing even one bit of information would release a tiny amount of heat, a figure that he calculated. This implies mitochondria are time machines because they also transform light energy into CO2, water, and heat = mtDNA is a hydrogen heat engine.
If information is energy, as Wheeler has told us, Information, once created, has to have a “finite and quantifiable mass.”
This connects information theory directly to energy and the mass equivalence equation of Einstein, E-mc^2.
This is how they are linked. Light is light energy in photon form.
HOW DOES THERMODYNAMICS LINK TO THE CIRCADIAN CLOCK?
How do cells do it? Your epigenetic mutation load (EML) of your tissues is the key to understanding how the light you use in your environment builds the life you live. Nature has built a clock timing mechanism as you live life based on your light choices. A higher EML has been associated with age-related pathological conditions like X chromosome activation skewing. The circadian clock in humans controls chromatin marking. BMAL1 is a clock gene, and HSF1 is a HEAT shock protein.
Remember what I said about Landauer’s principle above. As information is transfered, so is heat. This is why we have heat shock proteins in cells. Both get optimized by sunlight exposure. HSF1 is an important transcription factor for the induction of NAT1 in human cells and is required for androgen activation of the NAT1 promoter. This is why Neil Armstrong had lifelong problems with his testosterone levels when he returned from the moon, and it is why so many women struggle with sex hormone problems in their lives when they are filled with methylation problems from alien light. This is how humans inactivate the X chromosome to limit disease and create time. If we choose badly, the opposite occurs.
Shannon realized that the quantity of the message had ZERO to do with its true meaning. No one yet realizes the same thing is true in humans in how their colony of mitochondria works with sunlight.
Shannon found just using a “one and zero” is all it took to solve Bell Labs’ problems around understanding information = where the word “bit” comes from.
Physicist John Wheeler gave us the idea that everything is information.” = it from bit……..
Wheeler tells us every particle in the universe emanates from the information locked inside it.
Mitochondria are Turing machines that use Shannon’s binary code of 0 and 1, where 0 = H+ and 1 = deuterium, and solar photons drive the Boolean logic gates in the mitochondria to action. Mother Nature-innovation was profound. She created an electromechanical switching circuit that could decide things. She proved 3.8 billion years before Shannon that it was possible to perform complex operations by means of electromagnetic relay circuits built from hydrogen isotopes. I covered how mitochondria do this here ——-> https://optimalklubs.com/kruse-for-dummies-general/
NAD+/NADH is a proxy for melatonin production in our mitochondria by the rhythm and time of sunlight and by darkness in our lives we get. Melatonin is the key light hormone that protects the heteroplasmy rate mitochondrial DNA to keep clocks operating well. You won’t hear that from a food guru. This means melatonin is the photochemical gate keeper of the % of heteroplasmy in mitochondria in a cell. It not only controls inflammation (entropy) but it also controls turnover of DHA in the membranes of our cells. This complex dance begins in the skin and eye, at the RPE, where ocular melanin and melatonin begins its quantum magic by using AM light to regenerate the melanopsin receptors in broad daylight by using UV and IR light. They operate together when UV-IRA light are present simultaneously.
The spins of electrons/protons are not only manipulated by light. Light has both electric and magnetic fields. Spins of electrons and protons are also affected by magnetic fields (ATPase of mitochondria or the dynamo of Earth or those found in tech gear). It turns out spin states can also be affected by electrical fields (emitted from proteins side chains) and can be used to collect and store information optically from electrons or the photons they carry. This allows energy and information to be buried and included in the atomic structure of cells.
Brain entrainment through light pulsing hinges on synchronizing the brain’s electrical patterns with external stimuli. By emitting light at specific frequencies from mitochondrial metabolism, the brain is coaxed into a ‘frequency following response‘, aligning its brainwave patterns to the rhythm of the light.
This synchronization isn’t just fascinating; it’s profoundly useful from a physiological and evolutionary perspective. Our brainwaves mirror our mental states – beta waves dominate when we’re focused, while alpha waves signify relaxation. By entraining these frequencies with light, we can potentially steer our mental state, precisely guiding the cognitive ship.
The cellular organization is the key to precision optical signaling. Life is all about optimizing optical physics inside cells. It transforms energy from the environment to do this. Modern physics has now proven that energy and information are equivalent in physics. Landauer & Shannon’s work was critical in making this linkage.
The cellular organization is the key to precision optical signaling. Life is all about optimizing atomic molecular organization (AMO physics) INSIDE OF CELLS. It transforms energy into information from the environment. Modern physics has now proven that energy and information are equivalent in physics. Landauer & Shannon’s work was critical in making this linkage. Modern quantum biology has experimentally proven that energy is trapped directly at the electronic level in cells. Energy is stored not only as vibrational and electronic bond energies in biochemicals but also in the structure of the system: its membranes, gradients, fields and flow patterns, compartments, organelles, cell water, the size and shape of our ventricles, and tissues. All this, in turn, enables organisms to mobilize their energies coherently at any time it is needed and hence make available the entire spectrum of stored energies for physiological work. Life really is energy transformed on demand by Nature’s atomic design in cells. Light is the information powering the ENTIRE system.
SUMMARY
Who described the mathematics of decision-making? Claude Shannon did. Shannon showed how to map logic onto the physical world (ledger). Turing showed how to design computers in the language of mathematical logic.
Mother Nature pre-dated both men’s ideas by 3.8 billion years. Evolution was Nature’s laboratory that ended by creating a mitochondria which acts as a Turing machine.
Our brains need to optimally encode different options and compare between them. So, how did Nature build the brain? It created an organ filled with mitochondria that responds at an attosecond level to electric and magnetic fields at 90 degrees to each other in light waves. Our brain is measuring light waves to decipher the chaos in our environment. In an abstract way, it mimics the double-slit experiment in physics.
With this brain, decision making became more probable. During human decision-making, attention plays a pivotal role by guiding information sampling between alternative pathways in the brain’s mitochondria.
One of the hallmarks of the living system in cells is that they are exquisitely sensitive to specific, weak rhythmic signals.
During human decision-making, attention plays a pivotal role by guiding information sampling between alternative pathways in the brain. Our brains need to encode different options and compare them optimally using optics. So, how did Nature build the human brain? It created an organ that responds at an attosecond level to electric and magnetic fields at 90 degrees to each other in light waves. Our brain is measuring waves to decipher the chaos in our environment. It mimics the double-slit experiment in physics.
So far, the role of attention in decision-making has only been addressed through saccadic displacements in our eyes. Might saccade be the first clue that the brain is using our eyelids to episodically polarize unpolarized sunlight to create a new type of rhythm to make sense of our world? This NEW idea implies that seeing is not always attending, and attending is not always seeing.
Brain entrainment with light pulsing is more than a biological evolutionary advance. It might be the next frontier for neuroscientific technological advancement; it’s a window into peering into the vast potential of the human mind.
When Shannon met Turing
Computing fell in love
with digital information
A transformation
A revolution
New computations
Sparking innovations
When Shannon met Turing
a moment enduring
Alluring algorithms
touched information theorems
Man is way behind Mother Nature. Wolfgang Pauli realized that the free electrons in metal must obey the Fermi–Dirac statistics. Using this idea, he developed the theory of paramagnetism in 1926. Shortly after, Sommerfeld incorporated the Fermi–Dirac statistics into the free electron model and made it better to explain the heat capacity. Two years later, Bloch used quantum mechanics to describe the motion of an electron in a periodic lattice.
The mathematics of crystal structures developed by Auguste Bravais, Yevgraf Fyodorov, and others was used to classify crystals by their symmetry group, and tables of crystal structures were the basis for the International Tables of Crystallography series, first published in 1935. The band structure calculations were first used in 1930 to predict the properties of new materials, and in 1947, John Bardeen, Walter Brattain, and William Shockley developed the first semiconductor-based transistor, heralding a revolution in electronics.
Why did Nature innovate chlorophyll and hemoglobin before moving on to melanin in the evolutionary history of mammals? She learned that nitrogen and hydrogen could be liquefied under the right conditions and would then behave as metals. Then she had some solid-state physics she could innovate life with. Nature innovated the idea that a classical electron can move freely through a metallic solid in an aqueous liquid crystal. She realized the power embedded in anisotropic crystals, built us from them, and self-assembled them in sunlight’s electric and magnetic fields.
Birefringence is the optical property of a material with a refractive index that depends on light’s polarization and propagation direction. Birefringence occurs in anisotropic materials that are said to be birefringent. Piezoelectric materials, like bone or collagen,, are anisotropic; they do not have the same properties in all axes.
Is the ATPase ANISOTRPIC?
What do you know about phosphoresce and ATP? Is this important in creating the spectrum of biophotons from mitochondrial metabolism? Is this how it can vary? The answer is yes. Metabolism makes heat, light, CO2, and water. You do not see the light because mitochondrial matrix-created water is an electromagnetic capacitor for these bio-photons. The water is structured in coherent domains to be transformed for physiologically useful energy in a cell. This is the PoW mechanism at the core of the quantum cell.
In simple terms, phosphorescence is a process in which energy absorbed by a substance is released relatively slowly in the form of light. This is, in some cases, the mechanism used for glow-in-the-dark materials, which are “charged” by exposure to light.
Do you know that outside of the visible light spectrum, nnEMF causes calcium efflux? What is the effect of calcium efflux on the ATPase?
Did you know that the presence of excess calcium ions has been found to cause a 20% decrease in the phosphorescence emission anisotropy in a cell?
In centralized science, this is interpreted as being due to a conformational change in the protein based on the methodologies being studied. Moreover, it is supported by data from time-resolved phosphorescence measurements. These measurements also show a hard physical effect of nnEMF: nnEMF toxicity lowers the anisotropy.
Anisotropy is a basic property of all crystalline materials. Living tissue is anisotropic. The organism is a dynamic liquid crystalline continuum with coherent motions on every scale.
Even in nanocrystals and amorphous solids, e.g., metallic glasses, anisotropy is present on an atomic level. Therefore, magnetic anisotropy is an intrinsic property of magnetization in general.
For nanoparticles that are used in the quantum cellular design, this is hard to achieve: because of their small size, they are generally only slightly polarizable by light, and thus, the difference in potential energy will, for accessible electric fields, below. This implies that the conditions for alignment are specific and sensitive to electric fields in cells. Physics has shown that the minimum size to align a particle depends on the size and shape of the particle because of a nontrivial competition between particle bulkiness and anisotropy.
Anisotropy, denoted by lowercase “r” in physics equations, indicates molecular size, diffusion, and viscosity.
Several physical techniques or forces in nature can be employed to assist the self-assembly process in cells, such as alignment of the particles by introducing a substrate to the system (atoms), employing a fluid flow (viscosity), or applying external magnetic (free radicals) or electric fields (Becker’s DC). An external electric field can align an anisotropic particle due to its anisotropic polarizability, which causes the particle’s potential energy to vary with its orientation in the field present in cells. nnEMF changes this thermodynamic variable.
Since the thermal Brownian motion (Einstein’s most cited 1905 paper) competes with the tendency to align, the potential energy difference has to be high enough to overcome these fluctuations and substantially align the particle.
The dependence of the minimum size of an alignable particle on the shape ratio of the particle is non-trivial, as it is not in general true that for alignment, the more anisotropic the particle, the better, nor are bulkier particles always better: for all the particle shapes studied so far, the optimum shape lies in-between these variables. This implies abnormal Calcium movements in mitochondria have huge anisotropic effects in mitochondria. This larvae shows that effect below.
This change in the decay of the emission anisotropy is associated with only minor changes in the rotational relaxation time of the protein and is again suggestive of a conformational change in the protein. This means that one of the biological effects of nnEMF is an altered conformational change in protein semiconductors.
For example, muscle contractions reduce anisotropy; for instance, contraction of the quadriceps muscle can decrease anisotropy of the patellar tendon. If that muscle contraction is done under blue light, it compounds the effect inside of mitochondria.
In the brain anisotropy can be seen on MRI. Anisotropy measures describe the directional dominance of water diffusion within a region. Within a voxel, the anisotropy provides an index of the degree of uniformity of water diffusion for a specific orientation. Strongly directionally organized tissue, such as the corpus callosum, which is primarily comprised of tightly packed medial–lateral projecting fibers, has a high degree of anisotropy because there is a tendency for diffusion to be highly restricted along the fiber membranes to follow this medial–lateral direction.
However, when the callosal fibers intersect other pathways in the brain, such as the corticospinal tracts which control motor movement, this unidirectional organization is disrupted and the anisotropy is reduced. This has implications in diseases like ALS, Parkinson’s disease, and Alzheimer’s disease. Thus, there is a normal anatomy of the cerebral white matter of both high and low regions of anisotropy, and it is therefore not the case that greater anisotropy is always indicative of greater tissue integrity in human brain MRI. In fact, measurements of anisotropy have been performed for various brain diseases, and abnormalities (mostly reduction) have been reported.
In strokes of the human brain, diffusion tensor imaging shows an
increase in fractional anisotropy because of changes in the ATPase and mitochondrial response to hypoxia.
Welding fumes contain several metals, including manganese (Mn), iron (Fe), and copper (Cu) that at high exposure, may co-influence welding-related neurotoxicity. The relationship between brain accumulation of these metals and neuropathology, especially in welders with subclinical exposure levels, when compared with controls, welders had significantly lower fractional anisotropy in the globus pallidus where Parkinson’s Disease occurs.
SUMMARY
It was Albert Einstein who created the modern field of condensed matter physics, starting with his seminal 1905 article on the photoelectric effect and photoluminescence, which opened the fields of photoelectron spectroscopy and photoluminescence spectroscopy, and later his 1907 article on the specific heat of solids which introduced, for the first time, the effect of lattice vibrations on the thermodynamic properties of crystals, in particular the specific heat.
Condensed matter physics is the field of physics that deals with the macroscopic and microscopic physical properties of matter, especially the solid and liquid phases, which arise from electromagnetic forces between atoms and electrons. This field concerns itself with soft matter. This is the matter cells are made from.
Condensed matter physicists seek to understand the behavior of these phases by experiments to measure various material properties and by applying the physical laws of quantum mechanics, electromagnetism, statistical mechanics, and other physics theories to develop mathematical models and predict the properties of extremely large groups of atoms.
Anisotropy is firmly in the scientific realm of the condensed matter physicists. The diversity of systems and phenomena available for study makes condensed matter physics the most active field of contemporary centralized physics: one-third of all American physicists self-identify as condensed matter physicists.
Anisotropy is most typically examined using the calculation for fractional anisotropy (FA); described in Basser and Pierpaoli, 1996; applied in several manuscripts, e.g. Pfefferbaum et al., 2000; Abe et al., 2002), yet similar metrics such as relative anisotropy (RA) have also been applied in the diffusion-imaging literature examining lifespan changes (e.g. Huppi et al., 1998, 2001; Nusbaum et al., 2001; Miller et al., 2002; van Pul et al., 2005; Y. Zhang et al., 2005; Camara et al., 2007; Schneiderman et al., 2007; Stahl et al., 2007).
In some of the papers I have read on this fundamental process, ATP was also observed to lower the time-averaged phosphorescence anisotropy inside of cells, possibly via an interaction with the low-affinity regulatory site of the protein.
None of these things are controlled for in nnEMF toxicity studies. When my @Bitcoinandbeef interview
Cersosimo M. G., Koller W. C. (2006). The diagnosis of manganese-induced parkinsonism. Neurotoxicology 27, 340–346.
Lucchini R. G., Martin C. J., Doney B. C. (2009). From manganism to manganese-induced parkinsonism: A conceptual model based on the evolution of exposure. Neuromol. Med. 11, 311–321.
Hashimoto R., Mori T., Nemoto K., Moriguchi Y., Noguchi H., Nakabayashi T., Hori H., Harada S., Kunugi H., Saitoh O. (2009). Abnormal microstructures of the basal ganglia in schizophrenia revealed by diffusion tensor imaging. World J. Biol. Psychiatry 10, 65–69.
S. C. Glotzer and M. J. Solomon, Nature Mater. 6, 557 (2007).
S.-M. Yang, S.-H. Kim, J.-M. Lima, and G.-R. Yi, J. Mater. Chem. 18, 2177 (2008).
L. Rossi, S. Sacanna, and K. P. Velikov, Soft Matter 7, 64 (2011).
Watch the video above and head to daylightcomputer.com and use password KRUSE2023 to see more on this great innovation from Anjan Katta of Daylight Computer, based for now in San Francisco. Below is my receipt as the first customer of this innovation.
BLUE LIGHT IS A STIMULANT THAT CREATES ROS/RNS NORMALLY
And stimulants are 👍 great. Most Americans drink a few cups of stimulants each morning ☕️ to get themselves up to face the daily grind.
But you know what’s not great? Being stimulated 24 hours of every day by blue light. This ruins the dose-response curve of the ROS/RNS. That is precisely what is occurring to modern humans because they live indoors and use tech screens excessively. What else is different about this version of blue light? The blue light that wakes us up in the sun is NEVER present without 42% IR-A light, which is red light. AM sunlight has 42% red light in it and only 1600K of blue light. This small stimulus of blue light is about to improve the executive function of the prefrontal cortex. This blue light needs red light to control the oxidation ROS/RNS that blue light makes when it is present without red light in our light environment.
ALL CELLS contain ion channels in their outer (plasma) and inner (organelle) membranes. Like other proteins, Ion channels are targets of oxidative impact, which modulates ion fluxes across membranes. Subsequently, these ion currents affect electrical excitability, such as action potential discharge (in neurons, muscle, and receptor cells), alteration of the membrane resting potential, synaptic transmission, hormone secretion, muscle contraction, or coordination of the cell cycle.
An important class of ion channels is the family of potassium (K+) channels; they are not only in charge of the membrane resting potential or the repolarization of the action potentials but also control cell proliferation or transmitter/hormone release, to name a few. A subgroup of K+ channels are the so-called calcium (Ca2+) activated K+ channels, which need either an increase of Ca2+ at their intracellular face to open or a combination of Ca2+ and voltage to function correctly. Maxi Ca2+-activated K+ channels, also named BK channels, constitute a subgroup of Ca2+-activated K+ channels.
Do you know where these ion channels exist in humans? They are found on the inner mitochondrial membrane. EXCESSIVE BLUE LIGHT exposure destroys these potassium ion channels to ruin signaling of cells that control the circadian mechanism and are associated with leptin and melanopsin. LET THAT SINK IN.
Mitochondria are a significant source of ROS generation targeting BK channels. Blue light creates that stimulus when RED LIGHT IS ABSENT.
C TERMINAL CHANGES ARE A BLUE LIGHT STORY.
The inner membrane of mitochondria contains BK channels (mtBK), which appear essential in the production of ROS. mtBK channels appear to be inserted into the mitochondrial membrane with the toxin binding sites for charybdotoxin and iberiotoxin exposed to the mitochondrial intermembrane space. This can be accessed using outside-out patch configuration of the inner mitochondrial membrane. Consequently, the C-terminal tail domain, including the Ca2+ binding site, is localized to the mitochondrial matrix where the proton gradient exists.
RED LIGHT MOVES PROTONS BEST. Blue light creates the most ROS. Do you understand why subtracting red light and UV light from blue creates mitochondrial diseases now?
Your brain wakes up when you look at your computer or phone screen. It’s alert. Because it hears, “It’s daytime! Time to be focused and do human things!”
But guess when it’s terrible to hear that signal?
The other 14 hours of the day, the Sun wouldn’t usually send such a signal to the brain.
We need a break from the stimulus. Otherwise, we fry our circuits and get fatigued.
So take a break from the blue light our modern world worships. Stop the intravenous coffee to your SCN and allow yourself to relax.
WHY DO ALL HUMAN NEED THIS COMPUTER?
This computer builds your brain anabolically and does not destroy it catabolically as every other computer does.
WHY DOES ALAN (artificial light at night) or blue light cause melanoma?
Pyrimidine dimers are molecular lesions formed from thymine or cytosine bases in DNA via photochemical reactions. Ultraviolet light (UV) induces the formation of covalent linkages between consecutive bases along the nucleotide chain in the vicinity of their carbon–carbon double bonds. The dimerization reaction can also occur among pyrimidine bases in dsRNA (double-stranded RNA)—uracil or cytosine. Two everyday UV products are cyclobutane pyrimidine dimers (CPDs) and 6–4 photoproducts. Blue light causes these cyclobutane residues, which can lead to cancers like melanoma. Many people think UV light causes this, but blue light is way more potent in generating these melanoma-inducing chemicals, as shown below.
These pre-mutagenic lesions alter the structure and possibly the base-pairing in DNA. Up to 50–100 such reactions per second might occur in a skin cell during exposure to sunlight but are usually corrected within seconds by photolyase reactivation or nucleotide excision repair. Uncorrected lesions can inhibit polymerases, cause misreading during transcription or replication, or lead to arrest of replication.
Artificial man-made Blue Light “Enhances” Melatonin Suppression….via melanopsin damage………Imagine that?
🐭😱
I’m sorry, but we are still relatively close to the starting line when it comes to the amount of research into blue light and circadian rhythm so we kind of have to read what we have access to and do our best to be DIRECTIONALLY accurate in what we take from them and how they apply to humans.
This paper, however, is one of the best you’ll find anywhere.
They tested 24 humans. Some of whom, I’m told, actually look like mice.
They determined…
“Each fluence-response curve demonstrated that increasing corneal irradiances of light-evoked progressively increased nocturnal melatonin suppression. A comparison of these fluence-response curves supports the hypothesis that polychromatic fluorescent light is more potent for melatonin regulation when enriched in the short wavelength spectrum.”
Is there visual acuity flux in the human eyes due to variable factors in our light environment? Yes, there is. Black Swan MDs would be wise to recommend routine sunning the eyes to release stress in eye ciliary muscles to improve vision accommodation via dopamine modulation of the skeletal muscle fiber types in these eye muscles. Just knowing this data is true, one can’t help but wonder if prescription eyeglass wearers shouldn’t be evaluated in an eye doctor’s office over a series of days/times (diurnal exams) to account for these confounding lighting factors in determining overall average visual acuity. I’ve begun doing this for blue blockers. The results are quite interesting. It caused me to ask Anjan to build this computer. Blue locking glasses are not enough protection.
Based on my work with patients, a computer with zero blue light emission is the requirement. We will still need them for other things, but you won’t need them with Anjan’s computer.
There is a “revolution on the surface of the earth” called blue-lit technology, and it is causing a new evolution of free radical signals via nnEMF and magnetic fields from your environment, changing the internal terroir in your mitochondria, leading to diseases that appear to emerge from nowhere. Anjan’s computer puts a dent in this game plan hatched by Silicon Valley. This is why they want him to fail. The healthcare reality you obtain manifests from these collisions and creations.
SUMMARY
This conversation happened recently based on my work around decentralized medicine and anabolic computing in El Salvador.
Follow me closely with this, because this might be the most important post you read on Patreon in your entire life:
“I have known for years now that melatonin is anti-cancer. But every study I’ve read basically pegged it as such because of its antioxidant activities. This is true to an extent.
However, last night, a pretty brilliant neurosurgeon that I’ve been following for about five years now turned the light on in my mind and made it crystal clear to me precisely what the mechanism is that makes melatonin so crucial for cancer prevention and healing from cancer.
He made two statements:
1) blue (artificial) light, especially at night, causes cancer.
2) nnEMF (non-native electromagnetic fields – think cell phones, x-box, tablets, Wi-Fi routers, cell towers, smart meters, smart homes, Apple watches, Fitbit, Bluetooth, or anything that operates on wireless technology) causes cancer.
But here is the connection that he helped me make last night:
What is the hallmark trait of cancer? – dysfunctional cells that are like STEM CELLS that are multiplying and growing out of control in the body.
Here’s the rub: we ALL have cancer cells growing in our bodies. All of us. What makes it that one person doesn’t develop deadly cancers while others do?
One word: apoptosis. This describes the body’s innate ability to recognize a cell as dysfunctional and potentially cancerous and “orders” the cell to shut down and die.
The amount of melatonin controls apoptosis a mitochondrion can make, and our mitochondria make the most melatonin in our body. That amount is quantized to the light we live under.
If apoptosis works correctly in you, you will not develop cancer because your body can recognize those dysfunctional cells and neutralize them immediately. Problem solved.
Here’s the thing: MELATONIN, the hormone made in every mitochondria and found in our pineal gland created in the absence of LIGHT, regulates apoptosis. Let me make this plain as day for you (even if it is a crude description of a very complex biological process):
No melatonin = no apoptosis.
No apoptosis = dysfunctional cells growing out of control = CANCER.
Artificial light at night and nnEMF BOTH individually signal to your colony of mitochondria that it is daytime. In response, your colony of mitochondria and your pineal gland will dramatically reduce melatonin synthesis and output.
The light bulb was invented in the last 100 years, and homes across America have permanently changed how they live. What do we do when the sun goes down? We flip on the light switch and turn the computer. We sit on our phones. On our TVs and tablets. We are using iPads as digital babysitters!
All of this lowers our melatonin and arrests the process of apoptosis.
We are literally handcuffing our body’s natural and brilliant defense mechanism against cancer!
THINK ABOUT THIS FOR A MOMENT!
In our lifetimes, research shows that 1 in 2 of us will develop cancer. This is a VERY sharp rise from even 50 years ago.
We give money to cancer research charities, who then give that money to cash-rich pharma companies who don’t need our money so they can create drugs that don’t cure cancer and make us go broke using them. We run, walk, and bike for the cure.
What if the cure for cancer was right under our noses?
What if it’s as simple as shutting off the damn lights when the sun goes down? Use a computer that has zero blue light. We can all agree on using low amber lighting, wearing blue-blocking glasses, shutting off your Wi-Fi router, turning off your wireless devices, and instead of watching TV, hanging out and talking with your family and then going to bed early.
If it’s that simple to prevent cancer for you and your children, would you do it?
Below is a study that shows how melatonin regulates the apoptosis of cancer cells.
There are hundreds, if not thousands, of studies and research papers that show how artificial light at night suppresses melatonin and several studies that show how nnEMF does this as well.”
“Jack and Anjan might have solved one of the biggest riddles in the world. ”
Tumor immunity represents a new avenue for cancer therapy. Immune checkpoint inhibitors have successfully improved outcomes in several tumor types. In addition, currently, immune cell-based therapy is also attracting significant attention. However, the clinical efficacy of these treatments requires further improvement. The mechanisms through which cancer cells escape the immune response must be identified and clarified. Cancer stem cells (CSCs) play a central role in multiple aspects of malignant tumors. CSCs can initiate tumors in partially immunocompromised mice, whereas non-CSCs fail to form tumors, suggesting that tumor initiation is a definitive function of CSCs. However, the fact that non-CSCs also initiate tumors in more highly immunocompromised mice suggests that the immune evasion property may be a more fundamental feature of CSCs rather than a tumor-initiating property.
What if stem cells’ “evasion-by-replication” strategy were the root of cancer when they are hit by vaccine particles?
What If human cancer theory is upside-down?
In my Rubin Huberman podcast I told that it is upside based on the light story. It turns out it is upside down because of the SV-40 story uncovered by Sarah Stewart in the Cutter Incident too. How?
Cancer cells are actively looking for a source of UV light to control the cell cycle. Cells migrate when Ulraweak UV biophotons are absent from mitochondrial metabolism.
You’ll begin to see a new mitochondrial perspective of my advice. Transfecting immuno privileged stem cells with SV-40 is a bad idea with horrible consequences.
COVID-vaccine-induced cancer data from the Ethical Skeptic demonstrate cancer genesis isn’t necessarily a long inexplicable number of somatic mutations like Philip Buckholdts wants you to believe. Cancer genesis is contamination-induced and electromagnetic radiation increases contamination by DNA destruction which act as plasmids. The Covid aftermarket data now suggests 1 in 225 shots could trigger cancers.
People forget each octave of the electromagnetic spectrum has a particular energy associated with it and that energy links to how DNA is damaged. For example, DNA replication errors, especially those occurring at regions that are hard to replicate, are called fragile sites. These sites can cause breaks in DNA that results in pieces and parts of nDNA. This process alone can lead to cancer, primarily by making it more likely that fragments of chromosomes rearrange themselves, activating genes that lead to uncontrollable cell division. Mary Sherman and Sarah Stewart invented this science in their bio-weapons lab in New Orleans.
What is the target that these two women trip over with their use of the LINAC?
Cancers can be categorized into two groups: those whose frequency increases with age, and those resulting from errors during mammalian development. The first group is linked to DNA replication through the accumulation of genetic mutations that occur during proliferation of developmentally acquired stem cells that give rise to and maintain tissues and organs.
These mutations, which result from DNA replication errors as well as environmental insults, fall into two categories; cancer driver mutations that initiate carcinogenesis and genome destabilizing mutations that promote aneuploidy through excess genome duplication and chromatid missegregation. Increased genome instability results in accelerated clonal evolution leading to the appearance of more aggressive clones with increased drug resistance.
The second group of cancers, termed germ cell neoplasia, results from the mislocation of pluripotent stem cells during early development. During normal development, pluripotent stem cells that originate in early embryos give rise to all of the cell lineages in the embryo and adult, but when they mislocate to ectopic sites, they produce tumors. Light is capable of causing this mislocation. This is a transgenerational effect of the electromagnetic spectrum. The LINAC use showed this and that is why the SV-40 virus was made uber virulent by Sherman and Stewart work in New Orleans for the CIA.
Geminin is the target of the light spectrum in mammals to protect it from cancer.
Remarkably, pluripotent stem cells, like many cancer cells, depend on the Geminin protein to prevent excess DNA replication from triggering DNA damage-dependent apoptosis. Apoptosis is controlled by ultraweak UV light generation by mitochondrial metabolism. This link between the control of DNA replication during early development and germ cell neoplasia reveals Geminin as the target of light. Big pharma and oncology want to use geminin as a potential chemotherapeutic target in the eradication of cancer progenitor cells. Light is better than drugs because it has no side effects. All drugs carry the side effect risks. Oncology favors drugs because they are patentable for the profiteers they serve in centralized healthcare.
In centralized medicine & science there should be strict observation and questioning. This is key to finding a solution to a problem. They do not want to find a solution because it destroys the business model of oncology.
Observation: COVID vaccinations have already triggered many cancer, and a significant number of people have already died from cancer. Question: If supposedly viruses such as HPV trigger decades-long domino effect that leads to cancer, why do these vaccines accelerate it so much? Have we got it all wrong?
Observation: The mechanism of action of COVID vaccines is to penetrate a cell, hack it, have it produce a protein to trigger antibodies, but also to trigger a T-cell attack on the contaminated cell. Question: How come normal cells have survived that vaccine contamination and morphed so quickly into a cancerous cell?
Observation: When you dive into vaccine-induced case reports, you realize most vaccines are capable of triggering cancer. Question: How and why do different vaccine technologies, targeting different viruses or bacteria, all end up having the same effect? Isn’t there another more automatic process at play?
Cancerous cells have very distinct features that cannot be regained by normal cells over night. And the idea that any push genetic in any direction, would always end up with the same outcome is genetically or mathematically impossible.
So, what’s going on?
Centralized science in cancer believes the following: The majority of cancers result from random mutations arising during DNA replication in the normal stem cells required during development and tissue maintenance. Differences in cancer risk among different tissues can be explained by the total number of stem cell divisions in those tissues. Is this true based on the Covid data? It is not.
That means something else is behind the numbers. What is it?
SV-40 and the light you live in.
SUMMARY
Mammalian cancer cannot start in normal cells penetrated by vaccine particles, because these cells will be destroyed by the immune system MHC complex. The human immune system is highly efficient at clearing cancer cells via this mechanism. In humans, cancer can only be started in stem cell which are normally immune protected. So human cancer cells always have all the traits of a stem cell. That is not what centralized oncology believes. What a coincidence? Cancer theory was always upside down. And none of them knew that ultraweak UV bio-photons stimulate mitosis to get a stem cell out of normal immune protection. That implies UV light is the best chemotherapy one can have. It also means it is the best therapy to use in vaccine induced cancer and injury like long COVID.
I dislike Thanksgiving but I have a tradition where I retell my family the story of how the CIA used the artworld to change public opinion and this program was used to help assinate a president when it became clear that human perception could be harnessed by propaganda. Part of this story was retold to you in the podcast above. Here is the second part of the story for you to digest once you finish your Thanksgiving dinner today. I am warning you it may give some of you indigestion.
When I teach people about Bitcoin, I have two go-to stories about asymmetric values to explain how something worth so little can grow to something beyond your imagination. One is the Louisiana Purchase, and the other is Gertrude Stein’s experience with Picasso.
By 1905, Picasso became a favorite of American art collectors Leo and Gertrude Stein. Leo told his sister that his work would become iconic and valuable. She famously told Picasso I wouldn’t say I like your work, but I trust my brother’s eye for value. She began to collect Picasso’s early works for 5-20 dollars a painting. Today, some of those paintings are worth 400 million dollars in private peer-to-peer deals. These deals mimic the peer-to-peer network in Bitcoin. The value of Bitcoin has gone from 1 cent to 69,000 in 13 years.
Alice B. Toklas (pictured above on right) is remembered for being Gertrude Stein’s (left) great love and writing her unusual, revered memoir-disguised-as-cookbook chronicling their life together. On September 8, 1907, her first day as an American expat in Paris, Toklas met Stein. The two fell instantly in love and remained together for the next 39 years until Stein’s death in 1946.
After Gertrude died, her collection of 47 paintings (38 of which were by Picasso) was bequeathed to her nephew but remained on the walls of Toklas’s home. Gertrude’s nephew eventually passed ownership on to his three children, who decided to sell when Toklas died in 1967. Nelson Rockerfeller mother founded the Museum of Modern Art in NYC, and Nelson Rockerfeller was given the chance to buy from Stein’s collection first by the political powers that were in place at this time.
The number of MoMA-CIA crossovers is highly suspicious, to say the least when one reviews the history.
In the years since his death in 1973, Picasso’s stature as an artist elevated to the highest ranks, with some of his works going for more than $100 million in public auctions and reportedly at even higher sums in private deals. He remains the top-grossing artist at auction worldwide, raking $245 million across 3,400 lots in 2020 alone. He is, in many ways, today’s “Bitcoin Standard” of the art market.
For example, Picasso’s Delacroix-inspired Les femmes d’Alger ‘Version O’ (1955) for $179.4 million in 2015 to Steve Wynn.
Femme Assise, pictured above, sold for 63 million dollars. It depicts French artist and model Fernande Olivier, who went with Picasso to a remote village in Spain during the summer of 1909. While there, she posed for a number of his pictures.
PROPAGANDA AROUND ART WAS BORN IN TULANE UNIVERSITY’S MK-ULTRA
The Cold War was the most powerful macropolitical thing on the planet in the late 1940s and 1950s.
The CIA fostered and promoted American Abstract Expressionist painting worldwide for over 20 years. The USSR of Stalin post WW2 was about total centralization in all things. The CIA began experimenting with decentralization at this time in reaction to absolute centralization in the USSR.
The artists the CIA supported emphasize free, spontaneous, and personal emotional expression, and they exercise considerable freedom of technique and execution to attain this goal, with a particular emphasis laid on the exploitation of the variable physical character of paint to evoke expressive qualities (e.g., sensuousness, dynamism.) The CIA task was monumental because few Americans liked decentralized art in the 1950s. MK-ULTRA propaganda techniques were applied to change this perception. It was so successful that it also bleed into the CIA’s operations involved in the assassinations of JFK and RFK Sr.
This was a period when the great majority of Americans disliked or even despised modern art – President Truman summed up the popular view when he said: “If that’s art, then I’m a Hottentot.” As for the artists themselves, many were ex-communists barely acceptable in the America of the McCarthyite era of the 50s, and certainly not the sort of people usually likely to receive US government backing.
Who were the artists the CIA supported?
Clyfford Still, Theodoros Stamos, Jackson Pollock, Willem de Kooning, Arshile Gorky, Mark Rothko, Lee Krasner, Robert Motherwell, Franz Kline, Adolph Gottlieb, David Smith, Hans Hofmann, Joan Mitchell are a few.
The connection between the CIA and art is improbable until you know what MK-ULTRA was all about. Many of you heard about this program for the first time in my RFK Jr interview linked above.
This new artistic movement was propped up to be proof of the creativity, intellectual freedom, and cultural power of the US. Russian art, strapped into the communist ideological straitjacket, could not compete.
GENERAL GROVES GOT THIS IDEA FROM BERNAYS AND NAZI PROPAGANDA USED IN WW2
Many have forgotten General Groves was the most powerful man in the USA in WW2. He controlled the Manhattan Project from start to finish. He was the architect of the Cold War. He single handedly reversed the promise that FDR made to Stalin at Potsdam that the USA would rebuild Russia for the sacrifices Russia made in defeating the Nazi’s in Europe. The picture below is when FDR made this promise to Stalin right before FDR death.
Groves made sure that the DNC had replaced FDR’s Vice President before his fourth term so that Groves could control the power struggle that would result after Germany was defeated. Groves knew that FDR was sympathetic to Stalin. Groves wanted to limit emotion in post war politics because he realized that a chronic war was a powerful way to subvert the power in the executive branch. War allowed for emergency power to be instituted without much controversy. This allowed the industrial military complex to operate freely and covertly. General groves wanted this ability to continue after the war. Groves made sure the OSS office would become a central intelligence post in post war America by installing his own people. Dulles was his hand picked successor. Truman was Groves hand picked president because he could be easily manipulated by propaganda Groves created and the CIA propagated.
HOW DID THIS PROPAGANDA MACHiNE WORK IN THE ART WORLD?
The existence of this supportive policy in the art world in post war America, which had been rumored and disputed for many years, has now been confirmed for the first time by former CIA officials. Unknown to the artists, the new American art was secretly promoted under a policy known as the “long leash” – arrangements similar in some ways to the indirect CIA backing of the journal ENCOUNTER, edited by Stephen Spender.
The decision to include culture and art in the US Cold War arsenal was taken as soon as the CIA was founded in 1947 by Truman at General Groves’s request. This was how the industrial, military complex captured the executive branch of government in the USA. I covered this in the tweet thread cited below.
Dismayed at the appeal communism still had for many intellectuals and artists in the West, the new agency set up a division, the Propaganda Assets Inventory, which could influence more than 800 newspapers, magazines, and public information organizations at its peak. They joked that it was like a Wurlitzer jukebox: when the CIA pushed a button, it could hear whatever tune it wanted playing across the world.
The following key step came in 1950 when the International Organizations Division (IOD) was set up under Tom Braden. It was this office that subsidized the animated version of George Orwell’s Animal Farm, which sponsored American jazz artists, opera recitals, and the Boston Symphony Orchestra’s international touring program. Its agents were placed in the film industry, in publishing houses, and even as travel writers for the celebrated Fodor guides. And, we now know, it promoted America’s anarchic avant-garde movement, Abstract Expressionism in the art world.
Initially, more open attempts were made to support the new American art. In 1947 the State Department organized and paid for a touring international exhibition entitled “Advancing American Art,” with the aim of rebutting Soviet suggestions that America was a cultural desert. But the show caused outrage at home, prompting Truman to make his Hottentot remark and one bitter congressman to declare: “I am just a dumb American who pays taxes for this kind of trash.” The tour had to be canceled.
The US government now faced a dilemma. This philistinism, combined with Joseph McCarthy’s hysterical denunciations of all that was avant-garde or unorthodox, was deeply embarrassing. Many of you might have forgotten that RFK Sr worked under Joe McCarthy during these anti-communist times and this theme would come back to haunt the Kennedy family in November of 1963 and in 1968.
It discredited the idea that America was a sophisticated, culturally rich democracy. It also prevented the US government from consolidating the shift in cultural supremacy from Paris to New York since the 1930s. To resolve this dilemma, the CIA was brought in to change perception by using mind control techniques developed in the MK-Ultra program.
ALLEN DULLES WAS A GENERAL GROVES ACOLYTE AND HE WAS THE ARCHITECT OF THE KENNEDY DEATHS in 1963 and 1968.
ON APRIL 10, 1953, ALLEN DULLES became the newly APPOINTED DIRECTOR OF THE CIA, and he delivered a speech to a gathering of Princeton alumni. Though the event was mundane, global tensions were running high. The Korean War was coming to an end, and earlier that week, The New York Times had published a startling story asserting that American POWs returning from the country may have been “converted” by “Communist brain-washers.” This was classic Cold War propaganda born in the work of Edward Bernays. Dulles decided to use this technique on the people of the United States.
Some GIs were confessing to war crimes, like carrying out germ warfare against the Communists–a charge the U.S. categorically denied. Others were reportedly so brainwashed that they refused to return to the United States at all. As if that weren’t enough, the U.S. was weeks away from secretly sponsoring the overthrow of a democratically elected leader in Iran to install the Shah to gain control of the oil fields in the Middle East. The blow back of this CIA program would haunt future presidents.
DULLES EMPLOYED BERNAYS and GOEBBELS PROPAGANDA MACHINE ON THE US PUBLIC
Dulles had just become the first civilian director of an agency growing more powerful by the day, and the speech provided an early glimpse into his priorities for the CIA. “In the past few years, we have become accustomed to hearing much about the battle for men’s minds–the war of ideologies,” he told the attendees. “I wonder, however, whether we clearly perceive the magnitude of the problem, whether we realize how sinister the battle for men’s minds has become in Soviet hands,” he continued. “We might call it, in its new form, ‘brain warfare.’”
Dulles proceeded to describe the “Soviet brain perversion techniques” as effective but “abhorrent” and “nefarious.” He gestured to the American POWs returning from Korea, shells of the men they once were, parroting the Communist propaganda they had heard cycled for weeks on end. He expressed fears and uncertainty–were they using chemical agents? Hypnosis? Something else entirely? “We in the West,” the CIA Director conceded, “are somewhat handicapped in brain warfare.” This sort of non-consensual experiment, even on one’s enemies, was antithetical to American values, Dulles insisted, as well as antithetical to what should be human values. Behind the scenes Dulles was building a CIA program to mimic what the communists and Nazi’s had already done.
Newspaper headlines like “New Evils Seen in Brainwashing” and “Brainwashing vs. Western Psychiatry” offered sensational accounts of new mind-control techniques and technologies that no man could fully resist. The paranoia began to drift into American culture, with books like The Manchurian Candidate and The Naked Lunch playing on themes of unhinged scientists and vast political conspiracies. These current events in the newspapers were like a shark fin breaking the water, announcing to the public that the CIA had an active mind control program at the covert universities in the Deep South. This is why MK-Ultra was born and bred at Tulane University. I mentioned this in the RFK Jr Tetragrammaton podcast .
MK-ULTRA AT TULANE linked to museums, the media, and CBS
Three days after his speech decrying Soviet tactics, Dulles approved the beginning of MK-Ultra, a top-secret CIA program for “covert use of biological and chemical materials.” “American values” made for good rhetoric, but Dulles had far grander plans for the agency’s Cold War agenda.
MK-Ultra’s “mind control” experiments generally centered around behavior modification via electro-shock therapy, hypnosis, polygraphs, many forms radiation, artificial light and a variety of drugs, toxins, and chemicals. These experiments relied on a range of test subjects: some who freely volunteered, some who volunteered under coercion, and some who had absolutely no idea they were involved in a sweeping defense research program. From mentally-impaired boys at a state school to American soldiers to “sexual psychopaths” at a state hospital, MK-Ultra’s programs often preyed on the most vulnerable members of society.
The CIA targeted cities in the USA for testing as well. St Louis and SF were two of the best documented in this program. The CIA considered prisoners especially good subjects, as they were willing to give consent in exchange for extra recreation time or commuted sentences. Recall how they tested the SV-40 concentrated virus by the LINAC on an Angola death row inmate in August of 1963 to test their bioweapons to kill Castro. MK-Ultra gave birth to this program in the bioweapons lab run by Dr. Alton Ochsner (middle below) and Dr. Mary Sherman (second pic below).
Whitey Bulger, a former organized crime boss, wrote of his experience as an inmate test subject in MK-Ultra. “Eight convicts in a panic and paranoid state,” Bulger said of the 1957 tests at the Atlanta penitentiary where he was serving time. “Total loss of appetite. Hallucinating. The room would change shape. Hours of paranoia and feeling violent. We experienced horrible periods of living nightmares and even blood coming out of the walls. Guys turning to skeletons in front of me. I saw a camera change into the head of a dog. I felt like I was going insane.”
Bulger claimed he had been injected with LSD. Lysergic acid diethylamide, or acid, had become one of the CIA’s critical interests for its “brain warfare” program, as the agency theorized it could be useful in interrogations. In the late 1940s, the CIA received reports that the Soviet Union had engaged in “intensive efforts to produce LSD,” and that the Soviets had attempted to purchase the world’s supply of the chemical. One CIA officer described the agency as “literally terrified” of the Soviets’ LSD program, largely because of the lack of knowledge about the drug in the United States. “[This] was the one material that we had ever been able to locate that really had potential fantastic possibilities if used wrongly,” the officer testified.
All this went on right before the bioweapons program that began in the USA in New Orleans in 1950-1964. You need to understand the timeline of history to understand what is going on today in your world. Experiments with LSD was the precursor to the SV-40 experiments.
With the advent of MK-Ultra, the government’s interest in LSD shifted from a defensive to an offensive orientation. Agency officials noted that LSD could be potentially useful in “[gaining] control of bodies whether they were willing or not.” The CIA envisioned applications that ranged from removing people from Europe in the case of a Soviet attack to enabling assassinations of enemy leaders. On November 18, 1953, a group of ten scientists met at a cabin deep in Maryland’s forests. After extended discussions, the participants agreed that to understand the value of the drug truly, “an unwitting experiment would be desirable.”
ART AND MK-ULTRA MERGE
The connection between art and propaganda is not quite as odd as it might appear once you see it from this perspective. At this time, the new agency, staffed mainly by Yale and Harvard graduates, many of whom collected art and wrote novels in their spare time, was a haven of liberalism when compared with a political world dominated by McCarthy or with J Edgar Hoover’s FBI. If any official institution was in a position to celebrate the collection of Leninists, Trotskyites, and heavy drinkers that made up the New York School, it was the CIA.
Until now, there has been no first-hand evidence to prove that this connection was made, but for the first time, a former case officer, Donald Jameson, has broken the silence. Yes, he has said, the agency saw Abstract Expressionism as an opportunity, and it ran with it.
“Regarding Abstract Expressionism, I’d love to be able to say that the CIA invented it just to see what happens in New York and downtown SoHo tomorrow!” he joked. “But I think that what we did really was to recognize the difference. It was recognized that Abstract Expressionism was the kind of art that made Socialist Realism look even more stylized and more rigid and confined than it was. And that relationship was exploited in some of the art exhibitions.
“In a way, our understanding was helped because Moscow in those days was very vicious in denouncing any kind of non-conformity to its own very rigid patterns. And so one could quite adequately and accurately reason that anything they criticized that much and that heavy-handedly was worth support one way or another.”
To pursue its underground interest in America’s lefty avant-garde, the CIA had to be sure its patronage could not be discovered. “Matters of this sort could only have been done at two or three removes,” Mr. Jameson explained, “so there wouldn’t be any question of having to clear Jackson Pollock, for example, or do anything that would involve these people in the organization. And it couldn’t have been any closer because most of them were people who had very little respect for the government, in particular, and certainly none for the CIA. If you had to use people who considered themselves one way or another to be closer to Moscow than to Washington, well, so much the better, perhaps.”
This was the “long leash”. The centerpiece of the CIA campaign became the Congress for Cultural Freedom, a vast jamboree of intellectuals, writers, historians, poets, and artists which was set up with CIA funds in the early 1950s and run by a CIA agent. It was the beachhead from which culture could be defended against the attacks of Moscow and its “fellow travelers” in the West. At its height, it had offices in 35 countries and published over two dozen magazines, including Encounter.
SV-40 SIDEBAR OCCURING AT THE SAME TIME THE CIA WAS USING THE ART WORLD
The success of this program preconditioned the CIA to believe they could build a covert bioweapons lab in the USA and hide it below the noses of the public and keep it covert using propaganda. These same facades where used to link neo-con community of Ochsner to the gay underground community Clay Shaw and David Ferry were in New Orleans. This was how the CIA came to link the medical and gay community in the conspiracy to kill JFK. just look at the familiar links used in the art world via MK-Ultra and the ones I revealed in the RFK Jr podcast.
HOW DID THE CIA USE MODERN ART COVERTLY? IT CORRUPTED THE MEDIA AT THE SAME TIME
The Congress for Cultural Freedom also gave the CIA the ideal front to promote its covert interest in Abstract Expressionism. It would be the official sponsor of touring exhibitions; its magazines would provide useful platforms for critics favorable to the new American painting, and no one, the artists included, would be any the wiser.
This organization put together several exhibitions of Abstract Expressionism during the 1950s. One of the most significant, “The New American Painting,” visited every big European city in 1958-59. Other influential shows included “Modern Art in the United States” (1955) and “Masterpieces of the Twentieth Century” (1952).
Because Abstract Expressionism was expensive to move around and exhibit, millionaires, and museums were called into play. Nelson Rockefeller, whose mother had co-founded the Museum of Modern Art in New York, was pre-eminent among these. As president of what he called “Mummy’s Museum,” Rockefeller was one of the biggest backers of Abstract Expressionism (which he called “free enterprise painting”). His museum was contracted to the Congress for Cultural Freedom to organize and curate most of its important art shows.
The museum was also linked to the CIA by several other bridges that most of the American public is ignorant of. This is how the First Amendment of the United States was captured by the CIA.
William Paley, the president of CBS Broadcasting and a founding father of the CIA, sat on the members’ board of the museum’s International Program. John Hay Whitney, who had served in the agency’s wartime predecessor, the OSS, was its chairman. The Whitney museum of modern art sat on 75th and Madison Ave in New York City. I lived as a child in this neighborhood and was well aware of its history at an early age. Did you know that Tom Braden, first chief of the CIA’s International Organizations Division (IOD), was executive secretary of the museum in 1949?
Do you know who worked for William Paley in Dallas in 1963 and later became their network star?
Dan Rather used propaganda in his reporting to help his boss cover up the CIA operations that occurred 60 years ago yesterday.
Now dead, Mr Braden lived in Woodbridge, Virginia until 2009, in a house packed with Abstract Expressionist works and guarded by enormous Alsatians. He explained the purpose of the IOD.
Baden said, “we wanted to unite all the people who were writers, who were musicians, who were artists, to demonstrate that the West and the United States were devoted to freedom of expression and to intellectual achievement, without any rigid barriers as to what you must write, and what you must say, and what you must do, and what you must paint, which was what was going on in the Soviet Union. I think it was the most important division that the agency had, and I think that it played an enormous role in the Cold War.”
He confirmed that his division had acted secretly because of the public hostility to the avant-garde: “It was very difficult to get the 1950s anti-communist Congress to go along with some of the things we wanted to do – send art abroad, send symphonies abroad, publish magazines abroad. That’s one of the reasons it had to be done covertly. It had to be a secret. In order to encourage openness, we believed it had to be secret.”
If this meant that the CIA had to play the role of the Pope to this century’s Michelangelos, well, all the better: “It takes a pope or somebody with a lot of money to recognize art and to support it,” Mr. Braden said. “And after many centuries, people say, ‘Oh look! the Sistine Chapel, the most beautiful creation on Earth!’ It’s a problem that civilization has faced ever since the first artist and the first millionaire or Pope who supported him. And yet, if it hadn’t been for the multi-millionaires or the popes, we wouldn’t have had the art.”
Would Abstract Expressionism have been the dominant art movement of the post-war years without this CIA patronage? The answer is questionable to those outside the art world. Those inside of it would likely disagree. I have been of the opinion for a long time now, that it would not be wrong to suggest that when you look at an Abstract Expressionist painting, you are being duped by the CIA propaganda. Today, I am thankful to bring you this story I have told to my family at Thanksgiving because this year after the Tetragrammaton podcast with RFK Jr you can now fully understand how all the parts fit to explain US history the military wants you to forget.
But look where this art ended up: in the marble halls of banks, in airports, in city halls, boardrooms, and great galleries. For the Cold Warriors who promoted them, these paintings were a logo, a signature for their culture and system, which they wanted to display everywhere that counted. The CIA propaganda program succeeded in a big way.
The Covert Art Operation continues to bleed into the New Orleans bioweapons lab
In 1958, the touring exhibition “The New American Painting”, including works by Pollock, de Kooning, Motherwell, and others, was on show in Paris. The Tate Gallery was keen to have it next but could not afford to bring it over. Late in the day, an American millionaire and art lover, Julius Fleischmann, stepped in with the cash, bringing the show to London.
However, the money that Fleischmann provided was not his, but the CIA’s. It came through a body called the Farfield Foundation, of which Fleischmann was president, but far from being a millionaire’s charitable arm, the foundation was a secret conduit for CIA funds. This was how Ochsner got his LINAC from a Hill Burton Grant that the politicians who controlled the industrial military complex controlled in the 1950s. Amazing coincidence don’t you think?
So, unknown to the Tate, the public, or the artists, the exhibition was transferred to London at American taxpayers’ expense to serve subtle Cold War propaganda purposes. A former CIA man, Tom Braden, described how such conduits as the Farfield Foundation were set up. “We would go to somebody in New York who was a well-known rich person, and we would say, ‘We want to set up a foundation.’ We would tell him what we were trying to do and pledge him to secrecy, and he would say, ‘Of course, I’ll do it,’ and then you would publish a letterhead, and his name would be on it, and there would be a foundation. It was really a pretty simple device.” This is what the CIA did with Dr. Alton Ochsner in the 1950s after the Cutter Incident.
Julius Fleischmann was well-placed for such a role. He sat on the International Program of the Museum of Modern Art in New York board, as did several powerful figures close to the CIA. Many Americans in 2023 still do not know how art and the CIA were linked by propaganda.
The world today exists on a belief system that “those in power” can outrun the truth by using intelligence agencies and their technology by manipulating money in the art world – without consequences. The reality of the situation is that the world of art TODAY still is ruled by the consequences that CIA propaganda used to rehypothecate money to manipulate public opinion. They used the art world to create and steal money forever wars in the pre Vietnam era and today they are creating trillions of dollars in cancer patients to create massive piles of fiat money they can funnel from HHS to the DOD and CIA to run the chronic wars today.
MK-ULTRA DEMISE WAS AT THE HAND OF ANOTHER KENNEDY
In 1977, Senator Edward Kennedy oversaw congressional hearings investigating the effects of MK-Ultra. Congress brought in a roster of ex-CIA employees for questioning, interrogating them about who oversaw these programs, how participants were identified, and if any of these programs had been continued. The Hearings turned over a number of disturbing details, particularly about the 1953 suicide of Dr. Frank Olson, an Army scientist who jumped out of a hotel window several days after unwittingly consuming a drink spiked with LSD. Amid the growing criminalization of drug users, and just a few years after President Nixon declared drug abuse as “public enemy number one,” the ironies of the U.S.’s troubling experimentation with drugs appeared in sharp relief.
But throughout the hearings, Congress kept hitting roadblocks: CIA staffers claimed they “couldn’t remember” details about many of the human experimentation projects or even the number of people involved. The obvious next step would be to consult the records, but that presented a small problem: in 1973, amid mounting inquiries, the director of MK-Ultra told workers, “It would be a good idea if [the MK-Ultra] files were destroyed.” Citing vague concerns about the privacy and “embarrassment” of participants, the men who crafted MK-Ultra effectively eradicated the paper record for one of the United States’ most obviously illegal undertakings. A program born in secrecy would hold onto many of its secrets forever because the government covered its own illegal tracks.
SUMMARY
Remember what John D. Rockefeller promised Congress under the administration of Teddy Roosevelt that the Rockefeller family would bankrupt the US government one day for breaking up the Standard Oil Trust. The relationship between Modern Art and American diplomacy began during WWII when the Museum of Modern Art was mobilized for the war effort. MoMA was founded in 1929 by Abby Aldrich Rockefeller. A decade later, her son, Nelson Rockefeller, became president of the Museum. In 1940, while he was still President of MoMA, Rockefeller was appointed the Roosevelt Administration’s Coordinator of Inter-American Affairs. He also served as Roosevelt’s Assistant Secretary of State in Latin America.
The Museum followed suit. MoMA fulfilled 38 government contracts for cultural materials during the Second World War and mounted 19 exhibitions of contemporary American painting for the Coordinator’s office, which were exhibited throughout Latin America. Latin America is where Dr. Alton Ochsner made most of his fortune while he was alive. He offered medical sanctuary to all the dictators of Latin America.
This direct relationship between the avant-garde and the war effort was well suited: The term avant-garde began as a French military term describing vanguard troops advancing into battle.
In the battle for “hearts and minds,” modern art was particularly effective. John Hay Whitney, both a president of MoMA and a member of the Whitney Family, which founded the Whitney Museum of American Art, explained that art stood out as a line of national defense because it could “educate, inspire, and strengthen the hearts and wills of free men.”
Whitney succeeded Rockefeller as President of the Museum of Modern Art in January 1941 so Nelson could turn his entire attention to his Coordinator duties. Under Whitney, MoMA served as “A Weapon of National Defense.” According to a Museum press release dated February 28, 1941, MoMA would “inaugurate a new program to speed the interchange of the art and culture of this hemisphere among all the twenty-one American republics.”
The goal was “Pan-Americanism.” This was the environment that Dr. Alton Ochsner was operating in during the 1950s-60s during the Cutter Incident. Ochsner Medical Foundation Hospital had every Latin American flag outside of it for close to 40 years. I know because I saw them every day for 6 years of my residency in New Orleans.
A “Traveling Art Caravan” through Latin America “would do more to bring us together as friends than ten years of commercial and political work.”
When World War 2 ended, Nelson Rockefeller returned to the Museum, and his Inter-American-Affairs staffers assumed responsibilities for MoMA’s international exhibition program: René d’Harnoncourt, who had headed Inter-American’s art division, became the Museum’s vice president in charge of foreign activities. Fellow staffer Porter McCray became the Director of the Museum’s International Program.
Modern art was so well aligned with American Cold War foreign policy that McCray took a leave of absence from the Museum in 1951 to work on the Marshall Plan. In 1957, Whitney resigned his position as MoMA’s Chairman of the Board of Trustees to become United States Ambassador to Great Britain. Whitney remained a trustee of the Museum while he was Ambassador, and his successor as Chairman was… Nelson Rockefeller, who had served as Special Assistant to President Eisenhower for Foreign Affairs until 1955. Who was his VP? Nixon. Who is seated right next to Dr. Ochsner below? His policies began the The War on Cancer in 1971. This is another propaganda technique born at the same time the USD dollar was removed from the gold standard. You are all unaware of the tangled webs the CIA has woven to confuse you to get their agenda through.
In 1947, at the very moment that the Advancing American Art show was being recalled, and the United States Government was selling its O’Keeffe’s for fifty bucks a piece (all seventy-nine pieces in the show together brought in $5,544), the CIA was being created. The CIA grew out of “Wild” Bill Donovan’s Office of Strategic Services (OSS), which was the U.S.’s wartime intelligence apparatus. The OSS became the CIA and George H. Bush Father ran that office.
George W. Bush’s grandfather, the late US senator Prescott S. Bush, was a director and shareholder of companies that profited from their involvement with the financial backers of Nazi Germany.
The Guardian newspaper in the UK obtained confirmation from newly discovered files in the US National Archives that a firm of which Prescott S. Bush was a director was involved with the financial architects of Nazism. He worked directly with Joseph Goebbels the Nazi Propaganda chief. Imagine that.
His business dealings, which continued until his company’s assets were seized in 1942 under the Trading with the Enemy Act, has led more than 60 years later to a civil action for damages being brought in Germany against the Bush family by two former slave laborers at Auschwitz. This only caused a minor ripple in the US Press during his pre-election in 2000. Guess why? The media was already captured by his friends in the CIA decades before this controversy.
The evidence the Guardian found has also prompted one former US Nazi war crimes prosecutor to argue over 80 years ago that the late senator’s action should have been grounds for prosecution for giving aid and comfort to the enemy.
What is the evidence against the Bush family and their oil empire?
While there is no suggestion that Prescott Bush was sympathetic to the Nazi cause, the documents reveal that the firm he worked for, Brown Brothers Harriman (BBH), acted as a US base for the German industrialist, Fritz Thyssen, who helped finance Hitler in the 1930s before falling out with him at the end of the decade. We now have confirmed published evidence from US government archives that shows Bush was the director of the New York-based Union Banking Corporation (UBC) that represented Thyssen’s US interests and he continued to work for the bank after America entered WW2.
Bush was also on the board of at least one of the companies that formed part of a multinational network of front companies to allow Thyssen to move assets around the world.
Thyssen owned the largest steel and coal company in Germany and grew rich from Hitler’s efforts to re-arm between the two world wars. One of the pillars in Thyssen’s international corporate web, UBC, worked exclusively for, and was owned by, a Thyssen-controlled bank in the Netherlands. More tantalizing are Bush’s links to the Consolidated Silesian Steel Company (CSSC), based in mineral rich Silesia on the German-Polish border. During the war, the company made use of Nazi slave labor from the concentration camps, including Auschwitz.
The ownership of CSSC changed hands several times in the 1930s, but documents from the US National Archive declassified in 2003 that link Bush to CSSC, although it is not clear if he and UBC were still involved in the company when Thyssen’s American assets were seized in 1942.
Three sets of archives spell out Prescott Bush’s involvement. All three are readily available, thanks to the efficient US archive system and a helpful and dedicated staff at both the Library of Congress in Washington and the National Archives at the University of Maryland. You should fact check Uncle Jack.
The third set of documents, are also at the National Archives, are contained in the files on IG Farben, who was prosecuted for war crimes in Neuremberg.
A report issued by the Office of Alien Property Custodian in 1942 stated of the companies that “since 1939, these (steel and mining) properties have been in possession of and have been operated by the German government and have undoubtedly been of considerable assistance to that country’s war effort”.
Prescott Bush, a 6ft 4in charmer with a rich singing voice, was the founder of the Bush political dynasty and was once considered a potential presidential candidate himself. Like his son, George, and grandson, George W, he went to Yale where he was, again like his descendants, a member of the secretive and influential Skull and Bones student society. He was an artillery captain in the first world war and married Dorothy Walker, the daughter of George Herbert Walker, in 1921.
In 1924, his father-in-law, a well-known St Louis investment banker, helped set him up in business in New York with Averill Harriman, the wealthy son of railroad magnate E H Harriman in New York, who had gone into banking.
One of the first jobs Walker gave Bush was to manage UBC. Bush was a founding member of the bank and the incorporation documents, which list him as one of seven directors, show he owned one share in UBC worth $125. You may now understand why the Bush family favors a CBDC over Bitcoin now. You may also understand why the Bush family is no friend to anyone named Kennedy. They had a hand in JFK and RFK Sr. demises.
The bank was set up by Harriman and Bush’s father-in-law to provide a US bank for the Thyssens, Germany’s most powerful industrial family.
August Thyssen, the founder of the dynasty had been a major contributor to Germany’s first world war effort and in the 1920s, he and his sons Fritz and Heinrich established a network of overseas banks and companies so their assets and money could be whisked offshore if threatened again.
By the time Fritz Thyssen inherited the business empire in 1926, Germany’s economic recovery was faltering under Weimar hyperinflation. After hearing Adolf Hitler speak, Thyssen became mesmerized by the young firebrand. He joined the Nazi party in December 1931 and admits backing Hitler in his autobiography, I Paid Hitler, when the National Socialists were still a radical fringe party. He stepped in several times to bail out the struggling party: in 1928 Thyssen had bought the Barlow Palace on Briennerstrasse, in Munich, which Hitler converted into the Brown House, the headquarters of the Nazi party. The money came from another Thyssen overseas institution, the Bank voor Handel en Scheepvarrt in Rotterdam.
By the late 1930s, Brown Brothers Harriman, which claimed to be the world’s largest private investment bank, and UBC had bought and shipped millions of dollars of gold, fuel, steel, coal and US treasury bonds to Germany, both feeding and financing Hitler’s build-up to war. Interesting history lesson huh? I hope you do not choke on your turkey today.
Between 1931 and 1933 UBC bought more than $8m worth of gold, of which $3m was shipped abroad. According to documents now published in many books and FOIA requests, after UBC was set up it transferred $2m to BBH accounts and between 1924 and 1940 the assets of UBC hovered around $3m, dropping to $1m only on a few occasions.
In 1941, Thyssen fled Germany after falling out with Hitler but he was captured in France and detained there for the remainder of the war.
Mind you, there was nothing illegal in doing business with the Thyssens throughout the 1930s and many of America’s best-known business names invested heavily in the German economic recovery. This seems ironic when you see how the Biden administration treats corporations who do business with Russia today over Ukraine. The play book continues for the Deep State.
However, everything changed politically after Germany invaded Poland in 1939 because the covert plan could no longer stay hidden. Even then it could be argued that BBH was within its rights continuing business relations with the Thyssens until the end of 1941 as the US was still technically neutral until the attack on Pearl Harbor in 1941. The trouble started on July 30 1942 when the New York Herald-Tribune ran an article entitled “Hitler’s Angel Has $3m in US Bank”. UBC’s huge gold purchases had raised suspicions that the bank was in fact a “secret nest egg” hidden in New York City for Thyssen and other Nazi bigwigs. The Alien Property Commission (APC) launched an investigation. It turns out the Bush family did hide Nazi assets during the war. This is how the modern neo-cons were born in the US politics.
There is no dispute over the fact that the US government seized a string of assets controlled by BBH – including UBC and SAC – in the autumn of 1942 under the Trading with the Enemy Act. What is in dispute is if Harriman, Walker and Bush did more than own these companies on paper.
Erwin May, a treasury attache and officer for the department of investigation in the APC, was assigned to look into UBC’s business. The first fact to emerge was that Roland Harriman, Prescott Bush and the other directors didn’t actually own their shares in UBC but merely held them on behalf of Bank voor Handel. Strangely, no one seemed to know who owned the Rotterdam-based bank, including UBC’s president.
May wrote in his report of August 16 1941: “Union Banking Corporation, incorporated August 4 1924, is wholly owned by the Bank voor Handel en Scheepvaart N.V of Rotterdam, the Netherlands. My investigation has produced no evidence as to the ownership of the Dutch bank. Mr Cornelis [sic] Lievense, president of UBC, claims no knowledge as to the ownership of the Bank voor Handel but believes it possible that Baron Heinrich Thyssen, brother of Fritz Thyssen, may own a substantial interest.”
May cleared the bank of holding a golden nest egg for the Nazi leaders but went on to describe a network of companies spreading out from UBC across Europe, America and Canada, and how money from voor Handel travelled to these companies through UBC.
By September May had traced the origins of the non-American board members and found that Dutchman HJ Kouwenhoven – who met with Harriman in 1924 to set up UBC – had several other jobs: in addition to being the managing director of voor Handel he was also the director of the August Thyssen bank in Berlin and a director of Fritz Thyssen’s Union Steel Works, the holding company that controlled Thyssen’s steel and coal mine empire in Germany.
Within a few weeks, Homer Jones, the chief of the APC investigation and research division sent a memo to the executive committee of APC recommending the US government vest UBC and its assets. Jones named the directors of the bank in the memo, including Prescott Bush’s name, and wrote: “Said stock is held by the above named individuals, however, solely as nominees for the Bank voor Handel, Rotterdam, Holland, which is owned by one or more of the Thyssen family, nationals of Germany and Hungary. The 4,000 shares hereinbefore set out are therefore beneficially owned and help for the interests of enemy nationals, and are vestible by the APC,” according to the memo from the National Archives.
The Bush family was caught RED HANDED.
Jones recommended that the assets be liquidated for the benefit of the government, but instead UBC was maintained intact and eventually returned to the American shareholders after the war. Some claim that Bush sold his share in UBC after the war for $1.5m – a huge amount of money at the time – but there is no documentary evidence to support this claim. No further action was ever taken nor was the investigation continued, despite the fact UBC was caught red-handed operating a American shell company for the Thyssen family eight months after America had entered the war and that this was the bank that had partly financed Hitler’s rise to power.
The most sensational part of the story remains shrouded in mystery: the connection, if any, between Prescott Bush, Thyssen, Consolidated Silesian Steel Company (CSSC) and Auschwitz.
Thyssen’s partner in United Steel Works, which had coal mines and steel plants across the region, was Friedrich Flick, another steel magnate who also owned part of IG Farben, the powerful German chemical company.
Flick’s plants in Poland made heavy use of slave labor from the concentration camps in Poland. According to a New York Times article published in March 18 1934 Flick owned two-thirds of CSSC while “American interests” held the rest.
The US National Archive documents show that BBH’s involvement with CSSC was more than simply holding the shares in the mid-1930s. Bush’s friend and fellow “bonesman” Knight Woolley, another partner at BBH, wrote to Averill Harriman in January 1933 warning of problems with CSSC after the Poles started their drive to nationalize the plant. “The Consolidated Silesian Steel Company situation has become increasingly complicated, and I have accordingly brought in Sullivan and Cromwell, in order to be sure that our interests are protected,” wrote Knight. “After studying the situation Foster Dulles is insisting that their man in Berlin get into the picture and obtain the information which the directors here should have. You will recall that Foster is a director and he is particularly anxious to be certain that there is no liability attaching to the American directors.”
John Foster Dulles was the brother of Allen Dulles who JFK fired in 1961 after the Bay of Pigs. Coincidence?
Continuing the history lesson: But the ownership of the CSSC between 1939 when the Germans invaded Poland and 1942 when the US government vested UBC and SAC is not clear.
“SAC held coal mines and definitely owned CSSC between 1934 and 1935, but when SAC was vested there was no trace of CSSC. All concrete evidence of its ownership disappears after 1935 and there are only a few traces in 1938 and 1939,” says Eva Schweitzer, the journalist and author whose book, America and the Holocaust, was published in 2004.
Silesia was quickly made part of the German Reich after the invasion, but while Polish factories were seized by the Nazis, those belonging to the still neutral Americans (and some other nationals) were treated more carefully as Hitler was still hoping to persuade the US to at least sit out the war as a neutral country. Schweitzer says American interests were dealt with on a case-by-case basis. The Nazis bought some out, but not others.
The two Holocaust survivors suing the US government and the Bush family for a total of $40billon in compensation claim both materially benefited from Auschwitz slave labor during the second world war.
Kurt Julius Goldstein, 87, and Peter Gingold, 85, began a class action in America in 2001, but the case was thrown out by Judge Rosemary Collier on the grounds that the government cannot be held liable under the principle of “state sovereignty”.
Jan Lissmann, one of the lawyers for the survivors, said: “President Bush withdrew President Bill Clinton’s signature from the treaty [that founded the court] not only to protect Americans, but also to protect himself and his family.”
Lissmann argues that genocide-related cases are covered by international law, which does hold governments accountable for their actions. He claims the ruling was invalid as no hearing took place.
In their claims, Mr Goldstein and Mr Gingold, honorary chairman of the League of Anti-fascists, suggest the Americans were aware of what was happening at Auschwitz and should have bombed the camp.
The lawyers also filed a motion in The Hague asking for an opinion on whether state sovereignty is a valid reason for refusing to hear their case.
The petition to The Hague states: “From April 1944 on, the American Air Force could have destroyed the camp with air raids, as well as the railway bridges and railway lines from Hungary to Auschwitz. The murder of about 400,000 Hungarian Holocaust victims could have been prevented.”
The case is built around a January 22 1944 executive order signed by President Franklin Roosevelt calling on the government to take all measures to rescue the European Jews. The lawyers claim the order was ignored because of pressure brought by a group of big American companies, including BBH, where Prescott Bush was a director.
The US government and the Bush family denied all the claims against them.
In addition to Eva Schweitzer’s book, two other books were published in 2004-05 that raised the subject of Prescott S. Bush’s business history. The author of the second book, John Loftus, is a former US attorney who prosecuted Nazi war criminals in the 70s. At that time he lived in St Petersburg, Florida and earning his living as a security commentator for Fox News and ABC radio, Loftus worked on a novel which used some of the material he has uncovered on Bush. Loftus stressed that what Prescott Bush was involved in was just what many other American and British businessmen were doing at the time.
“You can’t blame Bush for what his grandfather did any more than you can blame Jack Kennedy for what his father did – bought Nazi stocks – but what is important is the cover-up, how it could have gone on so successfully for half a century, and does that have implications for us today?” he said.
Those implications lead right to the death of JFK and RFK Jr.
“This was the mechanism by which Hitler was funded to come to power, this was the mechanism by which the Third Reich’s defence industry was re-armed, this was the mechanism by which Nazi profits were repatriated back to the American owners, this was the mechanism by which investigations into the financial laundering of the Third Reich were blunted,” said Loftus, who is vice-chairman of the Holocaust Museum in St Petersburg. The US Treasury and Senator Warren wants you to believe in 2023 that Bitcoin is used to launder money when it is clear that this blog is laying the case out why rehypothecation of money is the strong suit of the CIA and all the people affiliated with them.
“The Union Banking Corporation was a holding company for the Nazis, for Fritz Thyssen,” said Loftus. “At various times, the Bush family has tried to spin it, saying they were owned by a Dutch bank and it wasn’t until the Nazis took over Holland that they realized that now the Nazis controlled the apparent company and that is why the Bush supporters claim when the war was over they got their money back. Both the American Treasury investigations and the intelligence investigations in Europe completely bely that, it’s absolute horseshit. They always knew who the ultimate beneficiaries were.”
“There is no one left alive who could be prosecuted but they did get away with it,” said Loftus. “As a former federal prosecutor, I would make a case for Prescott S. Bush, his father-in-law (George Walker) and Averill Harriman [to be prosecuted] for giving aid and comfort to the enemy. They remained on the boards of these companies knowing that they were of financial benefit to the nation of Germany.”
Loftus said Prescott S. Bush must have been aware of what was happening in Germany at the time. “My take on him was that he was a not terribly successful in-law who did what Herbert Walker told him to. Walker and Harriman were the two evil geniuses, they didn’t care about the Nazis any more than they cared about their investments with the Bolsheviks.”
What is also at issue is how much money Bush made from his involvement. His supporters suggest that he had one token share. Loftus disputes this, citing sources in “the banking and intelligence communities” and suggesting that the Bush family, through George Herbert Walker and Prescott, got $1.5m out of the involvement. There is, however, no paper trail to this sum.
The third person going who went into print in the early 2000s on this subject is John Buchanan, 54, a Miami-based magazine journalist who started examining the files while working on a screenplay. In 2003, Buchanan published his findings in the venerable but small-circulation New Hampshire Gazette under the headline “Documents in National Archives Prove George Bush’s Grandfather Traded With the Nazis – Even After Pearl Harbor”. He expands on this in his book – Fixing America: Breaking the Stranglehold of Corporate Rule, Big Media and the Religious Right.
In the article, Buchanan, who has worked mainly in the trade and music press with a spell as a muckraking reporter in Miami, claimed that “the essential facts have appeared on the internet and in relatively obscure books but were dismissed by the media as propaganda and Bush family as undocumented diatribes”.
One of the USAs oldest Jewish publications, the Jewish Advocate, has aired the controversy in detail in print. Review it at your leisure.
Please recall that President George W. Bush gave us the Patriot Act after “the emergency” of the Twin towers “happened”. I no longer think the Twin Towers was a terrorist action. I believe Bush pulled a play out from his family blue print.
George H.W. Bush, George W. father, also served as Director of Central Intelligence (DCI) from January 1976 to January 1977, just ten days shy of one full year. Though his tenure was limited, his accomplishments were many, and we are grateful to have served under his leadership. He became president after Ronald Reagan.
There is the link to Big Oil families who had a hand in killing the 35th President of the USA. MoMA’s John Hay Whitney and Thomas W. Braden were members of the OSS. The OSS became the CIA in 1947. Never forget what this criminal cabal has done and continues to do.
Game, Set, and Match.
That is conclusion of the RFK Jr interview you did not hear and what i said live on stage in Lisbon, Portugal.
8G mimics a car wreck to the human brain or an NFL LB hit to a QBs head. These situations induces brain trauma at a space time continuum. Nothing yet I have said is ground breaking to group of neurosurgeons. This post below is a groundbreaking mitochondrial medicine lesson.
Today’s lesson on biophysics of consciousness:
Light illuminates the reality of what time and space are to the human experience. Time and space are mere illusions of our perceptual abilities. If you use physical forces in Nature we can induce consciousness and we can make it disappear right before your eyes even as nothing on Earth really changes to prove this point. How? Watch the video. Time & space are constructs used by humans to better understand and operate in our world. That there is no such thing as an “external” and “internal” world and what we think we see “out there” is literally occurring and being conceived inside our head at the ATPase level.
Based on physics and biology, this science is unfortunately reality; it turns out that our ability to handle to use sunlight to handle the atomic mass in our ATPase that allows us to be consciousness. That sole ability that dictates all that we see and perceive in our world.
The colony of mitochondria in the human brain has a massive fleet of ATPase’s in it and the video above shows you how fast its physiology can be altered. The sunlight in the video did not change. The amount of deuterium in his head did not change. But the velocity his body flet did change and that change altered how the nanorotors operates in his head. He went from energy efficient to energy inefficient in a few seconds when the key environmental variables around light remained constant. There is a deep lesson in biophysics here.
Proof that this counterintuitive idea is true?
This is time lapsed photography of what happens in neurodegeneration in older humans that over decades. It does not have to take that long if the atomic mass is added at a faster rate in a younger brain. This young brain experienced the increased mass via momentum of the force of gravity induced by velocity and not the weight associated with the atomic mass of deuterium.
Deuterium’s higher atomic mass effectively mimics the increase G forces in your ATPase and your brain fails under that weight or mass. Consciousness declines to neurodegeneration and cognitive decline before your brain fails in death.
Anesthesia also induces this effect on our patients and we take it for granted and never study it. Do you know that strong magnetic fields induce unconsciousness in living things? Anesthesia induces dielectric and magnetic flux collapse.
SHARE IT.
Decentralized medicine has answers that centralized medicine whiff’s on.
Most people know about single nucleotide polymorphisms (SNPs) or single amino acid polymorphisms (SAPs), but few people ever get told how they operate in health and disease.
N-acyl amino acids in humans can involve acetylation, and C-terminus amino acids can be involved with methylation. Both are controlled by light. This post describes how the process happens.
Modifying the C-terminus of proteins is essential in understanding what light is doing biophysically to determine what biochemistry is possible in a cell. The C-terminus is also known as the carboxyl-terminus, carboxy-terminus, C-terminal tail, C-terminal end, or COOH-terminus. It represents the end of an amino acid chain (protein or polypeptide), terminated by a free carboxyl group (-COOH). When the protein is translated from messenger RNA, it is created from the N-terminus to the C-terminus. The convention for writing peptide sequences is to put the C-terminal end on the right and write the sequence from N- to C-terminus.
For example, while the N-terminus of a protein often contains targeting signals, the C-terminus can include retention signals for protein sorting. The most common Endoplasmic Reticulum retention signal is the amino acid sequence -KDEL (Lys-Asp-Glu-Leu) or -HDEL (His-Asp-Glu-Leu) at the C-terminus. This keeps the protein in the endoplasmic reticulum and prevents it from entering the secretory pathway in a cell.
For example, when the skin over the gut with a massive amount of POMC is not stimulated by solar light, POMC is lightly translated, and Vitamin D levels stay low. As a result, one form of C-terminal modification is prenylation. During prenylation, a farnesyl- or geranylgeranyl-isoprenoid membrane anchor is added to a cysteine residue near the C-terminus. Small molecular weight, membrane-bound G proteins are often modified this way. The circadian mechanism in cells operates via G proteins. With proper solar light, prenylation goes smoothly.
The enterocytes in the gut form a barrier. They include a mechanical boundary against pathogens, antigens, and toxins; the monolayer of intestinal epithelial cells (IECs) represents the human body’s largest contact area with the environment due to villi folding. From their early development in the crypt bottom until the shedding of aged cells at the villus tip, IECs follow a continuous turnover process. This process is controlled by the circadian mechanism in the SCN and transmitted to the gut via the peripheral nervous system and the melanin sheets in the organ of Zuckerlandl, where melanin and POMC reside.
Under physiological conditions, a complex interaction between cytoskeleton rearrangement and tight junction proteins guarantees that the cell shedding itself does not mean a disturbance of epithelial integrity. However, alterations of epithelial integrity lead to the development of gut inflammatory disorders, such as inflammatory bowel diseases (IBDs). IBDs are associated with marked alterations of IECs, leading to increased tight junction permeability, altered cytoskeletal rearrangement, and induction of epithelial cell death with a subsequent loss of barrier function. All IBDs are linked to poor solar exposure and or artificial light at night on the skin or via the eyes.
In Crohn’s disease, there is Rho-A prenylation, and the absent solar light then changes protein signaling in the enterocytes of the gut. This links epithelial homeostasis directly to intestinal inflammation.
The peptide created by POMC before cleavage is composed of three such segments: N-POMC, which is located at the N-terminus; ACTH, which is located in the middle; and β-LPH, which is located at the C-terminus. Each of these segments contains one MSH sequence: γ-MSH in N-POMC, α-MSH in ACTH, and β-MSH in β-LPH.
The N-terminus is also known as the amino-terminus, NH2-terminus, N-terminal end, or amine-terminus, is the start of a protein or polypeptide, referring to the free amine group (-NH2) located at the end of a polypeptide. Look at the structure of melanin below when it interacts with an electrophile metal.
When a protein is translated from messenger RNA, it is created from the N-terminus to the C-terminus. The amino end of an amino acid (on a charged tRNA), during the elongation stage of translation, attaches to the carboxyl end of the growing chain. Since the start codon of the genetic code codes for ONLY one amino acid, methionine, most protein sequences start with a methionine (or, in bacteria, mitochondria, and chloroplasts, the modified version N-formylmethionine, fMet). I wrote a blog on that topic on Patreon. You should have expected I told you this for a reason before the melanin story came out of my mitochondrial mist. The circadian mechanism operates 100% of the time in a posttranslational fashion. I laid out that case at the Palestra Health conference when I presented to several politicians and hedge fund managers who were present. Some proteins are modified posttranslationally, for example, by cleavage from a protein precursor and therefore may have different amino acids at their N-terminus. Light frequencies can change the N-terminus in proteins.
The N-terminus is the first part of the protein that exits the ribosome during protein biosynthesis. It often contains signal peptide sequences, “intracellular postal codes,” that direct the delivery of the protein to the proper organelle. The signal peptide is typically removed at the destination by a signal peptidase. The N-terminal amino acid of a protein is an essential determinant of its half-life. This is how the ubiquitin system operates, and quantum mechanics raises or lessens the probability of the likelihood of a protein being degraded. This is called the N-end rule.
The N-terminal signal peptide is recognized by the signal recognition particle (SRP) and results in the targeting of the protein to the secretory pathway. In eukaryotic cells, these proteins are synthesized at the rough endoplasmic reticulum. Protein N-termini can be modified co – or post-translationally. Modifications include the removal of initiator methionine (iMet) by aminopeptidases, attachment of small chemical groups such as acetyl, propionyl, and methyl, and the addition of membrane anchors, such as palmitoyl and myristoyl groups. There are many other N-terminus modifications like methylation. Light frequencies dictate how biochemistry unfolds.
N-terminus modification is how many diseases begin with aberrant light choices. Many pharmacological, genetic, and mechanistic studies in mammals have suggested that certain members of the N-acyl amino acids stimulate mitochondrial respiration and whole-body energy expenditure directly. Other complementary studies have also established roles for N-acyl amino acids in glucose homeostasis, adipogenesis, vascular tone, and bone homeostasis. This explains thoroughly why POMC has the protein construction it does.
The N-POMC is located at the N-terminus ACTH, which is away from the N and C terminus because it is located in the middle of the protein. This is a deep evolutionary clue about how mammals used ACTH to create sugar from light cleavage. What should shock you is that each of these cleavage segments contains one MSH sequence: γ-MSH in N-POMC, α-MSH in ACTH, and β-MSH in β-LPH. This tells you that light and dark are controlling the peptide’s cleavage.
Notably, the functional consequence and enzymatic regulation of each N-acyl amino acid in mammals highly depend on the structural properties of the fatty acid tail group and amino acid head group.
By integrating whole genome sequencing data with N-acyl amino acid levels, one can identify the EPIGENETIC determinants of N-acyl amino acid levels and cluster according to the amino acid head group. For example, in mammalian heart disease, this is why CYP4F2 is associated with many human cardiometabolic disorders. Centralized science has now identified the CYP4F2 locus as an epigenetic determinant of plasma N-oleoyl-leucine and N-oleoyl-phenylalanine levels in human plasma, as the papers below show. In experimental studies, it has now been demonstrated that CYP4F2-mediated hydroxylation of N-oleoyl-leucine and N-oleoyl-phenylalanine results in metabolic diversification and production of many previously unknown lipid metabolites in humans with varying characteristics of the fatty acid tail group, including several that structurally resemble fatty acid hydroxy fatty acids. These studies provide a structural framework for understanding the regulation and disease associations of N-acyl amino acids in humans and identify that the diversity of this lipid signaling family can be significantly expanded through CYP4F-mediated ω-hydroxylation.
Modern “centralized chemical biology” relies increasingly on protein chemistry, which ideally allows precise positioning of labels, cargoes, and post-translational modifications (PTMs) in the contexts of complex protein structures. The resulting modified proteins prove helpful in determining proper physiology and Big Pharma therapeutic applications. They allow us to understand the decentralized cell by the probing and modulating function, as well as their tracking and (un)caging in cells that happen with light and dark cycles.
Big Pharma chemists have developed various methods to control the convergent construction of site-selectively modified proteins. Traditionally, the non-site-selective chemical modification of proteins has relied on the nucleophilicity of the side-chains of natural amino acid residues like lysine (Lys) and cysteine (Cys), as well as protein N-terminus through direct acylation, alkylation and arylation with a wide array of electrophiles. In chemistry, an electrophile is a chemical species that forms bonds with nucleophiles by accepting an electron pair. Electrophiles accept electrons in biochemistry. Biological electrophiles are defined as electron-deficient species of chemicals that include heavy metals, environmental pollutants, toxic drug metabolites, flavor enhancers like Splenda, cell signaling mediators, and unsaturated aldehyde products of membrane lipid peroxidation.
When DHA is in the SN-2 position, it becomes planar. This is what turns the central retinal pathways of the retinohypothalamic tracts into a wide band gapped semiconductive LED array that targets melanin all over the brain. Melanin absorbs all light, ROS, and RNS to charge separate water to create a tremendous amount of electrons to power the system. In this illustration, electrons act as a canvas does in a painting: sunlight is the paint, and electrons are the brushes.
SUMMARY
BLUE LIGHT IS A STIMULANT THAT CREATES ROS/RNS NORMALLY
And stimulants are 👍 great. Most Americans drink a few cups of stimulants each morning ☕️ to get themselves up to face the daily grind.
But you know what’s not great? Being stimulated 24 hours of every day by blue light. This ruins the dose-response curve of the ROS/RNS. That is exactly what is occurring to modern humans because they live indoors and use tech screens excessively. What else is different about this version of blue light? The blue light that wakes us up in the sun is NEVER present without 42% IR-A light, which is red. AM sunlight has 42% red light and only 1600K of blue light. This small stimulus of blue light is about to improve executive function of the prefrontal cortex. This blue light needs red light to control the oxidation ROS/RNS that blue light makes when present without red light in our light environment.
ALL CELLS contain ion channels in their outer (plasma) and inner (organelle) membranes. Ion channels, similar to other proteins, are targets of oxidative impact, which modulates ion fluxes across membranes. Subsequently, these ion currents affect electrical excitability, such as action potential discharge (in neurons, muscle, and receptor cells), alteration of the membrane resting potential, synaptic transmission, hormone secretion, muscle contraction, or coordination of the cell cycle. Circadian biology controls all of this.
An important class of ion channels is the family of potassium (K+) channels (in the nitric oxide cycle); they are not only in charge of the membrane resting potential or the repolarization of the action potentials but also control cell proliferation or transmitter/hormone release, to name a few. A subgroup of K+ channels are the so-called calcium (Ca2+) activated K+ channels, which need either an increase of Ca2+ at their intracellular face to open or a combination of Ca2+ and voltage to function correctly. Maxi Ca2+-activated K+ channels, also named BK channels, constitute a subgroup of Ca2+-activated K+ channels.
Do you know where these ion channels exist in humans? They are found on the inner mitochondrial membrane. EXCESSIVE BLUE LIGHT exposure destroys these potassium ion channels to ruin signaling of cells that control the circadian mechanism and are associated with leptin and melanopsin. LET THAT SINK IN with all the ways modification happens on the C and N terminus of proteins. I only shared a couple with you in this blog.
Mitochondria are a significant source of ROS generation targeting BK channels. Blue light creates that stimulus when RED LIGHT IS ABSENT.
The inner membrane of mitochondria contains BK channels (mtBK), which appear essential in the production of ROS. mtBK channels appear to be inserted into the mitochondrial membrane with the toxin binding sites for charybdotoxin and iberiotoxin exposed to the mitochondrial intermembrane space. This can be accessed using outside-out patch configuration of the inner mitochondrial membrane. Consequently, the C-terminal tail domain, including the Ca2+ binding site, is localized to the mitochondrial matrix where the proton gradient exists.
RED LIGHT MOVES PROTONS BEST. Blue light creates the most ROS. Do you understand why subtracting red and UV light from blue creates mitochondrial diseases now?
Can you imagine what the centralized chemists controlled by Big Pharma may find when they look at C and N terminus modifications by light frequencies in POMC or DHA in humans?
CITES
1. Turner JR. Intestinal mucosal barrier function in health and disease. Nat Rev Immunol. 2009;9(11):799–809.View this article via: PubMed CrossRef Google Scholar
2. van der Flier LG, Clevers H. Stem cells, self-renewal, and differentiation in the intestinal epithelium. Annu Rev Physiol. 2009;71:241–260. View this article via: PubMed CrossRef Google Scholar
3. Watson AJ, Duckworth CA, Guan Y, Montrose MH. Mechanisms of epithelial cell shedding in the Mammalian intestine and maintenance of barrier function. Ann N Y Acad Sci. 2009;1165:135–142.
4. Long J.Z., Svensson K.J, Bateman L.A., Lin H., Kamenecka T., Lokurkar I.A. et al. The secreted enzyme PM20D1 regulates lipidated amino acid uncouplers of mitochondria. Cell. 2016; 166: 424-435
Centralized researchers say the processes behind the solar tracking are an unexpected mystery. Maybe if the knew the evolutionary history of flowers better they’d know about the history of the non visual photo receptive system?
Phototropins of plants and melanopsin or mammals have a lot in common. They are the blue light non visual photopigments. Auxin of plants and encephalopsin have a lot in common. I wrote about auxins in the Ubiquitination series years ago. What protects the nucleus from UV light in mammals? OPN3 = encephalopsin
Opsin 3 mediates UVA-induced keratinocyte supranuclear melanin cap formation in mammals. Opsins work with auxins too. Amazing Mother Nature reuses her best ideas huh?. Why don’t the scientists know? Because centralized science is done in silos.
The ancestors of flowering plants diverged from the common ancestor of all living gymnosperms before the end of the Carboniferous, over 300 million years ago. This is when mammals showed up on Earth as well and began to specialize in melanin biology and used opsins to expand its usefulness on Earth with a changing sun after the Cambrian explosion. In the Cretaceous epoch, angiosperms diversified explosively, becoming the dominant group of plants across the planet to create flowers. Without non visual photochemicals there is no flowering plants.
What do decentralized clinicians and scientists know? Light energy is known to mediate isomerization through several mechanisms, including thermal, photochemical, and mechanical effects. Photoactive molecules are often isomerized by photochemical action as they can directly absorb light exciting the molecules to an upper electronic state. In photoisomerization events, the photon energy of the electromagnetic radiation often causes the rearrangement of cis-trans positions of organic compounds that contain a double bond in their structure. See retinal transformation as a best in class example of this chemical process on Earth.
Decentralized medicine lesson: Earth’s atmosphere has not always contained significant amounts of oxygen. For the first two billion years of our planet’s history, the atmosphere was rich in carbon dioxide and methane, but around 2.4 billion years ago something changed: the Great Oxygenation Event that saw the abundance of free oxygen in our atmosphere dramatically rise. The cause of this is thought to be cyanobacteria, which are able to perform photosynthesis – the transformation of sunlight and carbon dioxide into metabolic energy to produce sugars that fuel life’s processes, and oxygen as a ‘waste’ product – using a green pigment called chlorophyll. I covered this in the Rubin/Kruse/Huberman Part 1 & Part 2 podcast.
I told Andrew that retinal predated chlorophyll, hemoglobin, and melanin, and that the retinal and chlorophyll evolved in tandem, absorbing sunlight at complementary wavelengths. That is biophysics 101.
Retinal-based phototrophic metabolisms are still prevalent throughout the world today, especially in the oceans where life began, and represent one of the most important bioenergetic processes on Earth. Recall that Andrew was surprised that mammalian brains where filled with amphibian melanopsin in the podcast, but I was not. I know the evolutionary history of the chemical evolution of light absorbing pigments.
Chlorophyll absorbs light peaking at wavelengths of 465nm and 665nm. This is why leaves appear green, because they reflect green light rather than absorb it. However, the Sun’s spectrum peaks at ~550nm, which includes yellow and green light.
A number of proteins that absorb sunlight contain a molecule of retinal, including one protein called bacteriorhodopsin that absorbs light peaking at 568nm, close to the wavelength at which the Sun’s light peaks, and most notably in the range that chlorophyll does not absorb in. This is exactly what should have gotten centralized science thinking that the two pigments – retinal and chlorophyll – co-evolved on early Earth before the sun emitted its increase burst of UV light around the Cambrian explosion.
Remember I told them both our sun is a G class star and I reminded them both of the implications of a changing light perspective? I retold this story to Bill Gifford in Part three of this podcast that has not yet been released. Here you are getting an early preview of that interview. I have argued for 15 years that because retinal is the simpler molecule and linked to every opsin found in mammals, it would have come first, with chlorophyll (which is more efficient at transforming sunlight into metabolic energy) evolving afterwards, with each filling different niches in terms of the light they absorb. This is why the biology of Vitamin A and Vitamin D are linked in mammals.
Experiments have now shown that combining bacteriorhodopsin with a membrane vesicle to form the equivalent of a biological proto-cell can effectively result in trapping and storing sunlight in a cell.
It should have made sense to centralized scientists that this was a very early evolutionary invention coinciding with the evolution of the first cells, but it was not because centralized biology does not understand how light sculpts life.
Today, in the lab, we now have proof my hunches years ago were correct. Using the energy-trapping capability of the cell membrane, the membrane potential [the difference in electrical potential between inside and outside the cell, allowing the cell to provide energy] represents one of the most important reasons why cells are the fundamental unit of life.
Because vegetation on Earth predominantly absorbs red light, but reflects infrared light, viewing vegetation using a spectroscope reveals a dramatic dip in reflected light at red wavelengths, a sudden decrease that is called the ‘red edge’. More complex animal life, like mammals also absorbs red light, but it is also absorbs infrared light as well. This gave animals more complexity at the same time in evolution. In plants, it has been shown today in NASA experiments that when probing the spectrum of light reflected from potentially habitable exoplanets, scientists could search for a red edge in the planet’s light, which would be a biosignature indicative of vegetation using chlorophyll, or its extraterrestrial equivalent. This red edge also explains why the picture below is axiomatically true and why you must question your centralized eye doctors.
SUMMARY
I’m back in NYC right now and am visiting the place where I figured this out as a youngster. Today I am back at the Hayden Planetarium on the West side of Central Park with all the leaves changing color because of a changing light cycle. When light changes it induces a light stress in the plant. This is seen by us a color change in leaves. Similarly, when mammals are stressed by light they exhibit a blue shift in their non visual photoreceptive system. This has huge implications fro decentralized clinicians learning how to care for their patients in the new paradigm of medicine I am bringing to the government of El Salvador.
In Malibu and again on stage in Lisbon Portugal I made the case that the mRNA vaccines gave humans who were compliant with the vaccine mandate blue shifted. When their tissues were blue shifted, the non visual photoreceptors were damaged, retinal was released, and photonic signal was changed and this lead to sudden and new complications in our clinics. I knew to expect this in March of 2020 and this is why I told my tribe to avoid these new genetic therapies.
How did I figure this out as a kid? My time at the Hayden Plantetarium as a kid was critical in answering this mystery. I was curious about light and how the sun changed over eolutionary timescales and remember that I was taught in grade school sunflowers use retinal in them. I then engaged my curioity further and I found out that retinal absorbs what green plants reflect back to the environment. This is why all plant life looks green to the mammalian eye. This is another perfectly couple system in biology on Earth that links absorption and emission spectra of light.
Intriguingly, since retinal pigments in the mammalian eye and in the non visual photosystems absorb green and yellow light, and reflect or transmit red and blue light, then retinal-based life, early on Earth would have appeared purple in color if humans were on Earth to see it.
THE COLOR PURPLE SOLVED THE MYSTERY
Proteobacteria are the oldest bacteria on Earth in our evolutionary history. They are a purple bacteria. Proteobacteria are the dominant prokaryotes in aquatic systems. The ocean is where life begain. The Proteobacteria lineage contains phototrophs, chemolithotrophs, and chemoorganotrophs, and its members can be found in both oxic and anoxic environments.
This explained to me why they were the dominant form of life on Earth before the Great Oxygenation event.
Since retinal (Vitamin A) is a much simpler molecule than chlorophyll, I reasoned, it could and should be more commonly found in life in the Universe, and therefore a ‘green edge’ in a planet’s spectrum potentially should be viewed as a biosignature for retinal-based life. It turns out now NASA agrees with Uncle Jack too. They always look for the green reflected edge of planets spectra now when they are looking for life in the cosmos. The non visual photoreceptor system is a key in the development of the melanin in the mammalian system on Earth. Chalk one up for decentralized science over the centralized opinions.
NOW YOU SHOULD UNDERSTAND WHY ALL THESE PICTURES I HAVE USED FOR YEARS WHERE WAY AHEAD OF THEIR TIME.
I was just out in Malibu with Mr. Rubin and one of his friends, interviewing me for a movie we are making about me and Quantum Biology. We sat down two days ago and did a three-hour podcast that will be part 3 of the Tetragrammaton series. The goal of part 3 is to go deeper into the implications of what was said between Rick, Huberman, and me. Part 3 was done without Andrew. Bill Gifford sat in his place, and he is an award-winning health journalist.
SO WHAT DID WE TALK ABOUT?
Can we see the evidence of light toxicity in the skin before it afflicts the brain? Yes, we can. People often forget that the skin and brain come from the same tissue layers in the human embryo. Because of this linkage, your skin and your eyes tell your decentralized physician to look deeper into your health to see how badly you are afflicted with light toxicity. See this thread and read my comments for the details. HYPERLINK
Do you know the implications of the last post above about breast cancer and Vitamin D and sulfation? What happens when you add sunlight to a skin? Melanin becomes eumelanin because of the addition of the sun. Did your experts know that? Did you see the color of all human hair, skin, and eyes is made from this sulfated semiconductor? Do your experts know how this all works in the human mammal? I’m just warming up, folks.
What makes melanins so unique and so attractive to science these days?
The list of arguments is a long one. From the viewpoint of physicochemical properties, all melanins share:
(a) a broadband absorption spanning the entire spectral range of the visible domain
(b) a permanent electron paramagnetic resonance (EPR)d signal denoting a stable paramagnetic character.
An unpaired electron can change its electron spin by either absorbing or emitting a photon of energy, denoted by hv, such that the resonance condition, hv = the change in Energy is obeyed. This leads to the fundamental equation of EPR spectroscopy.
Electron Paramagnetic Resonance (EPR) is the study of direct transitions between the electronic Zeeman levels of the ground state. EPR is a magnetic resonance method under suitable microwave stimulation, enabling the unpaired electrons by their magnetic moment. The basic concepts of EPR are analogous to those of nuclear magnetic resonance (NMR), but the spins excited are those of the electrons instead of the atomic nuclei.
(c) hydration-dependent semiconductor-like behavior. For example, eumelanin conductivity increases in water because it conducts electricity via ions and electrons.
(d) efficient dissipation of electromagnetic energy as heat. Melanins can absorb massive amounts of light and get rid of it quickly without damage to the system. Water with a high dielectric constant helps facilitate this.
On the chemical side, most melanins display:
(a) antioxidant properties, both as an H-atom donor and as a reducing agent;
(b) metal chelation and binding of organic compounds
(c) redox behavior.
In addition, melanins are bioavailable, biocompatible, and biodegradable, thus representing the most promising candidates for biomedical applications in optical signaling in the condensed matter physics world of science.
Melanin has many of the same semiconductive abilities we see in cytochrome c oxidase, which is also a semiconductive protein (above). That protein is responsible for water creation in the mitochondrial matrix. Water creation and alteration by the mitochondrial matrix is how the DC electric current is stepped down to the precise amperage to create the regenerative drafts used in mammalian tissue regeneration found by Robert O. Becker’s experiments..
Melanin is the critical tissue in all mammals. It allows for tissue engineering and regeneration via nanotechnology operations in the cell via a combined diagnosis and therapy (theranostics) action with our stem cell supply. Melanins are also critical in creating the bio-photon spectrum needed to run the specificity of biomolecules in the cellular system of control. The source of the electromagnetic wave spectrum has to match the absorption spectra of biomolecules to keep the system far from equilibrium so coherence and entanglement are possible.
WHAT IS INFLAMMATION IN THE MAMMALS FUNDAMENTALLY?
It is from a lack of sun or too much light at night. This is the primary decentralized cycle in all of biology.
Eumelanin is a form of melanin and conducts electricity – albeit weakly – in its natural state. Researchers first discovered that the polyindolic pigment was a semiconductor in the 1970sand suggested that this behavior comes from energy bands associated with a non-localized empty molecular orbital within the eumelanin polymer chain. All free radicals are paramagnetic because they have unpaired electrons. So are all the melanins in mammals. This makes them the ideal wide band gapped (WBG) semiconductor to absorb them. This again points out how modern biology is lost in the woods. They believe ROS/RNS is terrible when, in fact, they are critical in how non-linear optical signaling controls biochemistry in cells by creating the right spectrum in bio-photon release from tissue-level metabolism controlled by mitochondria. When melanin is missing, chaos in tissues is created = inflammation. That is how inflammation manifests in you and every mammal on this planet. This is how modern neolithic disease is being made in the USA at alarming rates.
So, my patrons, I hope you are beginning to see why Nature wants to limit deuterium in the mitochondrial matrix now. Could its carburetor function be linked to water chemistry that is quantized to the amount and spectral density of biophoton release in the matrix by metabolism?
I think so.
A lack of POMC, degraded melanin, and a matrix not making water is all a sign of a mammal in deep need of the sun to begin its melanin renovation Rx.
Well, it turns out that deuterium in the mitochondrial matrix is controlled differently in every body tissue because each tissue needs a specific regenerative current to differentiate stem cells to rebuild tissues anew.
The reason is simple: deuterium concentration allowed into the mitochondrial matrix is how a cell controls metabolic rates in different tissues. No two tissues have the same physiology. Therefore, metabolic rates have to vary in these tissues to be thermodynamically efficient. This creates the spectrum of the VUV-IR-A light used to manage the biochemistry in that specific tissue. Not all tissues have the same metabolic rates because of their physiologic needs. This means the metabolism of a mitochondrion produces its unique spectra. A unique spectrum means the matter in these tissues must also have individual absorption spectra. This should raise the question, how does the matrix in differing tissues get more deuterium? What type of WBG semiconductors should we expect there? What is the gating mechanism?
The answer is the type of melanin adjacent to the uncoupling proteins of mitochondria that generate heat from metabolism. Remember, all haplotypes produce varying amounts of heat via uncoupling efficiency. The thermodynamics here are also linked to how badly degraded the melanin is in the tissue system. A big clue to this mystery is if ROS/RNS production is driving biomolecules of inflammation higher or lower: HS CRP, haptoglobin, homocysteine, lowered glutathione, procalcitonin, etc. This heat is liberated into the surrounding water to dampen the current in the electrical conduction pathways found in cells.
The recently released Owen Sheasby podcast illuminated this effect.
The further one goes from the equator; the more uncoupling humans need to use to control the regeneration current in a tight ampere range. Equatorial light is the most powerful light on Earth, and this is the light human mammals evolved under. That system is a powerful melanin stimulus for the skin. At higher latitudes, cold temperatures stimulate more robust frequency endogenous light generation. Moreover, as a result, more heat is produced, and melanin in our interiors becomes a better electrical conductor. Any excess heat is thermalized directly to water so the system can remain far from equilibrium. The slide at the beginning of this blog post shows this effect.
The closer the equator one lives, the less uncoupling one needs because the sun provides all the ingredients for self-regulated autophagy and apoptosis, which is controlled by ferroelectric currents in the cell that are dampened by melanin biology. Why is ferroelectricity the key to this process?
Iron’s toxicity is mediated by sunlight, and few people seem aware of it. Please recall the first steps of heme synthesis in mammals begin in the mitochondria. This was proven by papers from Simcox JA, Mitchell TC, Gao Y, et al. In Rubin, Kruse, Huberman Part 1 & @ I told you hemoglobin was the second big innovation in evolution after chlorophyll.
Heme synthesis begins its first step in mitochondria. If you have a circadian mismatch disease tied to melanopsin dysfunction by definition you are blue light toxic or nnEMF toxic and this causes a defect in mitophagy and ruins the iron cycle in humans. This immediately affects the liver clocks, too. This leads to fatty liver disease.
People in centralized healthcare often forget heme synthesis occurs partly in the mitochondria and partly in the cytoplasm. This is precisely how the TCA and urea cycle are built in us too. The process begins in the mitochondria because one of the precursors is found only there. Since this reaction is regulated in part by the concentration of heme, the final step (which produces the heme) is also mitochondrial.
People with defects in iron always have a blood dyscrasia (anemia) at some level and it usually bleeds into fertility and thyroid hormone creation too, because of its link to AM sunlight deficiency. These pathways are proximal to the melanin-building pathways as the slide shows below. In Part 3, I get into it with Bill about how melanin degradation and bleeds backward into this pathway via hypoxia. This is a catabolic effect All nnEMF cause hypoxia in humans and drives this catabolism of endogenous melanin to lead to interior destruction and a lack of wound healing.
Remember, purple light = UV light and it creates oxygen in our venous blood and this drives anabolic pathways to make melanin via POMC and alpha MSH.
Purple light in sunlight ALSO stimulates RBC synthesis in humans. Blue light causes RBCs to break down sooner and live a shorter life than they can. What is the color of the main breakdown color of heme? It is the complementary yellow color of bilirubin. Yellow is the complement of purple, and orange is the complement of blue in the color wheel.
An analogy to explain this idea is how paragliders use the thermals on Mount Blanc to ride high up into the atmosphere. The sun heats the air at the mountain’s base, and the heat rises to carry the gliders to very high altitudes. This allows them to ride the thermals almost at no energy cost. The only price needed is the solar input that drives the temperature variations. If you were a glider who wanted to go further than anyone else has ever gone, you’d need to add an engine to your back that could work to power a fan to move you further. If you did this, you’d have to have a solution for the altitude problem. Why? As we go higher, oxygen is not as expected, and neither is temperature. This is why the circadian mechanism measures them in their optical lattice clock mechanism. I explained this to Mr. Sheasby in his podcast and the Tetragrammaton part 3 podcast. This is why the human retina consumes more oxygen than any tissue in the human body. Modern eye researchers and clinicians do not explain why the choriocapillaris does what it does. I realized it immediately as the source of why obesity happens when the periphery of the retina is destroyed by blue light. This also occurs when melanopsin is at its highest density in human tissues. The choroid sits adjacent to the retinal pigmentum epithelium on its densely fenestrated side to act like a radiator to absorb heat. A thickening of the choroid is the first sign of impending obesity in humans (Pics below). BOOM
This also explains why fat people now have lousy bones and why the mechanical stress of weight no longer makes Wolf’s law factual in centralized biology.
Metabolomics network studies show that the kinetic isotope effect (KIE) of deuterium affects the metabolism of L-lysine, L-glutamine, and L-serine. This is why linoleic acid loaded with deuterium affects bone metabolism at its core. Pass that fact on to the food gurus. They remain ignorant of biophysics. Be careful who packs your parachute, folks.
As such, you’d need a mechanism to alter the fuel and oxygen mix to be oxidized to power your flight. This is very similar to what a car has to do with its carburetor. The higher you go, the more pseudohypoxic you get, so you must alter the fuel source to maintain your flight. The third through fifth citations below highlight this.
Mitochondria are hydrogen-fueled engines, so deuterium concentration and production is critical in biology. This explains the title of this paper. Deuterium-depleted water stimulates GLUT4 translocation in the presence of insulin, which leads to decreased blood glucose concentration. I still chuckle at the food gurus ranting about seed oils and never realizing they are deuterium bombs. https://pubmed.ncbi.nlm.nih.gov/34510301/
The UCP-2 proteins were innovated for this reason. It controls the fuel-oxygen mix in mitochondria. It is a carburator for deuterium/H+ flow. The more deuterium that flows in, the more anions in the TCA cycle are bound to the substrates because of the kinetic isotope effect (KIE) of deuterium. One deuteron binds 96 H+ protons in the matrix. This slows the spin rate of the TCA cycle. That has an indirect effect of raising and lowering methionine in its metabolic cycle, causing a collection of heavy metals. This is how melanin detoxes heavy metals and does not use endogenous glutathione. When someone has heavy metal toxicity, it is a sign to me, as a decentralized clinician, that they have a vast POMC problem and they need more sunlight to renovate melanin inside the affected tissue. Chelating with exogenous agents is a losing strategy of functional medicine. The reason it’s so popular is because of the revenue it generates.
SUMMARY
How do you know your clinician is genuinely a decentralized mitochondriac? The whole world will tell you they are nuts, and you should not follow what they tell you. Be wise enough to know that the paradigm does not like truth-tellers. They are bad for business.
Is melanin a perovskite material with unique biophysical abilities that centralized biology has ignored at your peril? You bet your ass it is. What else doesn’t centralized science know? Biophysics controls all the biochemistry in their books. If you do not understand what light is doing you don’t understand decentralized biochemistry either. They are light ignorant. Biomacromolecular pigments, such as melanin, play an essential role in the survival of all living beings as I told Rick and Andrew. Melanin absorbs sunlight transforms it into heat and deposits the energy in water and proteins at the electronic level to build a dissipative system. This step is crucial for avoiding damage to skin cells. Light absorption produces excited electrons, which could either fall back to ground states by releasing the heat (photothermal effect) and/or light (photoluminescence), or stay at higher energy levels within its lifetime period, which can be captured through external electronic circuitry (photovoltaic effect). In published studies that no one in centralized biology reads, it has been demonstrated that the combination of melanin with halide perovskite light absorber in the form of a composite exhibits high absorbance from the UV to NIR region in the solar spectrum. And the hybrid displays significantly reduced photoluminescence and minimized density of residual excited states (verified by photovoltaic measurement) owing to the enhanced considerably nonradiant quenching by the melanin.
As a result, the composite shows an ultrahigh solar-thermal quantum yield of 99.56% and solar-thermal conversion efficiency of ≈81% under one-sun illumination (AM1.5), which is superior to typical carbon materials such as graphene (≈70%). By coating the photothermal composite film on the hot side of thermoelectric devices, a 7000% increase in output power as compared to the blank device under illumination is observed. Mammals are experts in collecting the sun using this technology woven into the fabric of NATURE. Get your skin in the game of the sun.
Please remember blue light induces hypoxia in cells, and this stimulus causes melanin to break down into L-DOPA, dopamine, adrenalin, and noradrenaline. Every biochemistry textbook printed has this pathway, but most centralized PhDs and clinicians have no idea how it links to melanin biology. How much crowd wisdom is there when most of the crowd is afflicted by nnEMF and blue light, and their frontal lobes have been emptied of melanin/L-DOPA/dopamine anyway?
More sun = more water production by the mitochondrial matrix = more mitochondrial melatonin production = less chance of leptin resistance = less chance of neolithic disease. Any light at night causes leptin resistance = Blue light at night is the worst offender = because it makes melatonin vanish = causing leptin resistance = mitochondriac, and melanopsin wisdom and proves the food guru fail……
LIGHT’S EFFECT > FOOD EFFECT
All food is, at its core is matter created downstream from sunlight—photosynthesis wisdom on display. When the world moves away from your biological necessities, becoming fearful is fruitless. That’s not the point, given the dire situation. It’s learning how to control your fear, harness it, and use it as fuel to change your conditions of existence. Fear shouldn’t shut us down; it should wake us up to increase the fidelity of our awareness and focus to overcome the present challenge we face and crush it.
Stand for what is right even if you are standing alone. There is a fine line between challenging yourself and overwhelming yourself. Changing paradigms is not for the weak of heart or mind. This type of transformation takes hold of you. Invades you. Soon it owns you. You want to be free of them, but you never will be. A prolonged movement on the right way is better than overwhelming speed on the wrong path, and this is why you enjoy the chaos of being overwhelmed. You must become the change you seek in this world now.
Part 3 of Tetragrammaton is epic. I hope you all enjoy it once Mr. Rubin is done editing it.
HAPPY HALLOWEEN!
CITES
1. Pullman, A., and Pullman, B. (1961). The band structure of melanins. Biochim. Biophys. Acta. 54, 384–385. doi: 10.1016/0006-3002(61)90389-4
Schwarzschild’s equation is used to calculate radiative transfers. These are energy transfers that occur via electromagnetic radiation through any medium in local thermodynamic equilibrium that both absorbs and emits light radiation.
The general theory of relativity states that in particular, the curvature of spacetime is directly related to the energy and momentum of whatever matter and radiation are present.
Einstein’s general theory of relativity can be summed up in just 12 words:
Space-time tells matter how to move; matter tells space-time how to curve.
This also implies that light energy responds to the action of matter.
The Schwarzschild equation and the Schwarzschild radius are related concepts in the theory of general relativity, which describes how gravity affects space and time. The Schwarzschild equation is a mathematical solution to the Einstein field equations, which describe how the curvature of space-time depends on the distribution of mass and energy. Noether’s theorem solves the energy requirements of the bending of space and time.
I actually talked about that here in this podcast but I think few people really understood where Uncle Jack was driving you.
Many smoothed brain thinkers believe everything is just about energy with respect to the mass equivalence equation. They do this because they have a rudimentary understanding that equation. This concept offers us nothing, as I’ll explain below.
WHY THE OWEN SHEASBY PODCAST NOT YET RELEASED WILL MATTER DEEPLY TO THOSE WHO REMAIN IN THE DARK
If you consider the mass-energy equivalence relationship, E= mc^2 you might be led to this conclusion. However, what this equation really tells us is that matter is not conserved in Nature. It is a shocking because it tells us that mass can be converted to energy. It does say how but Nature allows for it. In other words, E=mc^2 tells us something deep about mass that has huge implications for biology. That’s why it’s useful to the mitochondriac. However the concept that everything is just energy gets us nowhere in terms of understanding our world. It is essentially a statement of existence. The fact that the universe exists and is full of energy is an empirical fact. It is not explained by the concept of energy. Similarly, the laws of physics are ultimately empirical, and they are also not explained by energy. Energy is essentially an accounting tool that helps us solve problems. This is what leptin is in biology. Melanin however, is a lot like Noether’s theorem. It tells us a lot about the mass in the system and how much light can be absorbed into the system. The physics is given in the nature and character of the fundamental forces that describe how things interact.
Life is basically about electricity and magnetism that come from light in a system. Think about the tests done by your centralized doctor in the form of an EKG, EEG, and an EMG. All show the electrical and magnetic potential of our organ systems. Anything and everything electrical stems from the phenomena of charge. No one seems to have a clue why this relationship in nature exists, but physics tells us it is true. Atoms are made up of 3 parts: Protons have a positive charge, neutrons are neutral, and electrons have a negative charge. Here is the interesting part: Electrons have the equal and opposite charge of protons, but an electrons atomic mass is 1/1836th that of a proton. This is a huge difference in mass. Thusly, charge of these particles is the main variable with respect to their atomic mass. Atomic mass links to the thermodynamics and energy needed in the system because mass determines the size and shape in protein lattices. The charge of the lattice is determined by the protons and electrons in the system. Electrons delocalize most often because they are not encumbered by the mass as protons are. This points out why deuterium is a problem in mitochondrial biology. The mass of the lattice determines the how the speed of light can travel in our tissues. It also determines the frequency of light emitted. This is the basis of how a semiconductor emits light = LED.
The speed of light is variable in a substance when it becomes encumbered by electrons. This is why size and shape alter the thermodynamics of things made up of electrons and protons. Light only interacts with electrons via the photoelectric effect. Thusly, electrons are exicted and powered up by light. Light instantaneously interacts with matter to create the fastest pathway through tissues. This directly links tissues to Fermat’s principle. Light does not interact with protons or neutrons and has to go around them. This increases the distance that light must travel and it creates tiny delay’s in tissues at the quantum level. Just because the distance increases does not mean the path is longer in all cases. That small delay creates a signal that denotes biologic time in a cell. That delay is observed in the telomere length of a cell. What moves atoms or things made up of atoms? Light is capable of this fundamental task and nothing else can.
How light is captured and travels in our tissues is how time manifests in biology = melanin biology.
On the flip side; energy and momentum are quantities that will crop up in the analysis of virtually all physical systems that exhibit such symmetries. Noether’s theorem says that every symmetry implies a conservation law is present and acting and that link is always to energy in the system in question.
For mammals, melanin controls that process.
THE PICTURE STORY ABOVE SHOWS YOU CENTRALIZED SCIENCE STILL HAS NO IDEA HOW FAR AHEAD MY MEMBERS ARE IN THE STORY OF LIGHT AND MAMMALS.
Understanding the physics of organisms is the only way to resolve this chasm in knowledge.
Light has a universal speed limit at 186,000 miles an hour in space where matter is sparse compared to space-time. Inside a cell matter is not sparse. Light travels 30 centimeters in one nano-second. The only way to increase its energy/power is to increase its frequency and this is why endogneous light production is a key feature improvement in mammals. That change in energy can alter the electric and magnetic fields associated with the atomic lattice present in cells where matter is present. When those fields are altered, so are the interactions that can occur with specific light frequencies. The frequency of light determines the current and the force of the current. The DC current is what determines wakefulness and sleep. Current is the flow of electrons or protons inside the matter of cells and is measured in amperes. During daytime the DC current is present and at night it is absent in the brain when we sleep.
Magnetic fields are produced by the motion of electrical charges inside of tissues. A fundamental property of magnetic fields is that they exert forces on moving electrical charges. Magnetism is best seen in cells by the free radicals they create as they move electrical charges inside of cells.
Magnetism outside of cells is best visualized by putting a magnet under a paper and throwing iron filings on the paper. You can see the field the magnet generates by looking at the pattern of the iron filings. If you throw away the filings and add new iron filings the exact same pattern will emerge showing you that the magnet, and not the atoms of iron, determine the shape of the field of action. This action is very similar to what the human body undergoes every night and day cycle. Its molecules are disturbed by daylight constantly and are condensed back to their form at night. Sunlight alters, disturbs, and un-condenses magnetic fields. Sometimes atoms in us are lost and we have to replace them from our environment. We get a fresh supply of atoms from water, food, and from light. But thanks to the controlling forces within our cells, namely our mitochondrial electric and magnetic fields, new molecules and cells are rebuilt as before and arrange themselves in the same pattern as old atoms were. They are recycled by autophagy and apoptosis in our colonies of mitochondria.
Current has another feature called electromotive force. This is the “push” behind the current and it is measured in volts. Currents in space flow differently than they do on Earth. This is a function of the plasma they exist in. Plasma is one of the four fundamental states of matter, the others being solid, liquid, and gas. A plasma has properties unlike those of the other states of matter. Plasma in space can travel multi-directionally. Plasma’s inside the ionosphere can only flow unidirectionally. The presence of a significant number of charge carriers makes plasma electrically conductive so that it responds strongly to electromagnetic fields. Like gas, plasma does not have a definite shape or a definite volume unless enclosed in a container or contained by an environment. Unlike gas, under the influence of a magnetic field, it may form structures such as filaments, beams and double layers. In space, current flows in all directions because space is essentially a vacuum filled with double layered plasmas. The ionosphere itself is a plasma. Sunlight must traverse that plasma to get to mammals.
On Earth, within the ionosphere where life exists, energy flows unidirectionally from the sun to the surface of the Earth. This flow controls the quantum yield of photosynthesis which forms the basis of the food webs on Earth. Current only flows when a source of electrons is connected to a conductor that contains fewer electrons. This is why lightening (another plasma) flows from clouds to the Earth’s surface and not into space. This allows flow from things with a higher electron density to one with a lower density of electrons. If there is no conductor present between these density changes in electrons, there is only a hypothetical charge of flow we call the electric potential. That potential is measured in volts.
An electric field forms around any electric charge and we can now imagine them with unrivaled precision. That implies that any other charged object if it has an opposite polarity, will be attracted. If the charge is similar they will be repelled. The charge differentially is reflected in the distance between the two densities. The distance between to charged particles is called an electric field. The field is the region of the space of this plasma in which an electric charge can be measured. This is measured in volts per unit of area. All electric fields are associated with magnetic field actions by Maxwell’s laws. We can distinguish electric fields from magnetic ones easily today. This was not true in our recent past.
Charge is poorly understood by most people. Understanding of magnetism, by most, is atrocious. Magnetism is an intrinsic property of atoms that manifests in two polarities. Any flow of electrons is accompanied by a combined electric and magnetic field around the current of flow of electrons. Those two fields are always at 90-degree angles to one another. As electrons flow, they disturb other electrons around them in these fields. Just as a current produces a magnetic field, a magnetic, when it moves in relation to a conductor, induces a current. Magnetic fields are measured in Gauss. Both fields are determined by lines of force and they indicate the direction and shape of the field locally between particles. Both fields power declines with distance but their influence over charged particles is infinite.
SUMMARY
General relativity has acquired a reputation in centralized scinece as a theory of extraordinary beauty. Why? Subrahmanyan Chandrasekhar has noted that at multiple levels, general relativity exhibits what Francis Bacon has termed a “strangeness in the proportion” (i.e. elements that excite wonderment and surprise). It juxtaposes fundamental concepts (space and time versus matter and motion) which had previously been considered as entirely independent. Chandrasekhar also noted that Einstein’s only guides in his search for an exact theory were the principle of equivalence and his sense that a proper description of gravity should be geometrical at its basis, so that there was an “element of revelation” in the manner in which Einstein arrived at his theory just by thinking about the Universe. Other elements of beauty associated with the general theory of relativity are its simplicity and symmetry, the manner in which it incorporates invariance and unification, and its perfect logical consistency. But there is a problem.
Reconciliation of general relativity with the laws of quantum physics remains a huge problem in modern science. As a mitochondriac you must hold open the idea that Einstein is wrong in some of his assumptions. Why? Mother Nature operates quantum mechanicallly 100% of the time. I trust her more than Sir Albert. Not only that, Einstein also doubted his own work when he introduced the cosmological constant.
Quantum mechanics is the science of probabilities, biology is the study of the improbable which only makes sense from the perspective that the living state is only probable using reactions that appear statistically improbable. The power in that sentence is immense and highlights the difference in understanding between the decentralized and centralized science.
WHY DON’T I TRUST A SCIENTIST I REVERE?
He is centralized in his ideas.
You should know that the Einstein field equations are nonlinear and are very difficult to solve. Einstein used approximation methods in working out initial predictions of the theory. But in 1916, the astrophysicist Karl Schwarzschild found the first non-trivial exact solution to the Einstein field equations. This was called the Schwarzschild metric.
This solution laid the groundwork for the description of the final stages of gravitational collapse, and the objects known today as black holes. In the same year, the first steps towards generalizing Schwarzschild’s solution to electrically charged objects were taken, eventually resulting in the Reissner–Nordström solution, which is now associated with electrically charged black holes. In 1965 -75 Einstein’s predictions in general relativity were proven again correct when quasar black holes were found to exist in nature. This tells us his theory has deep predictive value, but it still does not jive with quantum mechanics…….the science of biology.
In 1917, Einstein applied his general theory of relativity to the universe as a whole, initiating the field of relativistic cosmology. This is where I think he went off the rails. In line with contemporary thinking, he assumed a static universe, adding a new parameter to his original field equations—the cosmological constant—to match that observational presumption. By 1929, however, the work of Hubble and others had shown that our universe is expanding. This is readily described by the expanding cosmological solutions found by Friedmann in 1922, which do not require a cosmological constant. Lemaître used these solutions to formulate the earliest version of the Big Bang models, in which our universe has evolved from an extremely hot and dense earlier state. Einstein later declared the cosmological constant the biggest blunder of his life. He knew there was a fly in his own ointment.
Why does all this matter to us, as Black Swan mitochondriacs?
In the study of heat transfer, Schwarzschild’s equation is used to calculate radiative transfer (energy transfer via electromagnetic radiation) through a medium in local thermodynamic equilibrium that both absorbs and emits radiation. I use this daily when I am calculating what the effect of nnEMF is on me in a particular zipcode when I am traveling. I am on my way to Europe today.
When solar radiation is scattered it creates the phenomena that makes the sky appear blue to your brain. For example, scattering from clear skies reflects about 32 W/m2 (about 13%) of incoming solar radiation back to space.
Visible light is also reflected and scattered by aerosol particles and water droplets (clouds). Neither of these phenomena have a significant impact on the flux of thermal solar infrared through clear skies.
You need to be bathing in that light chronically. If you do not and use man made light to bath in I would expect one of two things to afflict you:
1. A mitochondrial disease inflicted by the SCN on your colony of mitochondrial in some tissue linked to the leptin melanocortin pathway because of how our system is built to work in decentralized fashion. People forget that the ipRCGs are directly wired to the SCN.
2. A mental disorder or neurodegenerative condition because of how the leptin melanocortin pathways wire directly to the habenular nucleus without any synapses. Today’s blog helps explain why ALL MENTAL ILLNESSES links to the physics of light. If you have one of these diseases or you know someone who has a history of these diseases, you should immediately jump to the conclusions at some level in their life or their transgenerational existence, that their cells lines have been afflicted by horrible choices around light to ruin the neurotransmitters created in their brain. They do not have a chemical deficit that requires a pharmaceutical deficit. They suffer from a solar light deficit and/or an artificial light addiction present day or night or both.
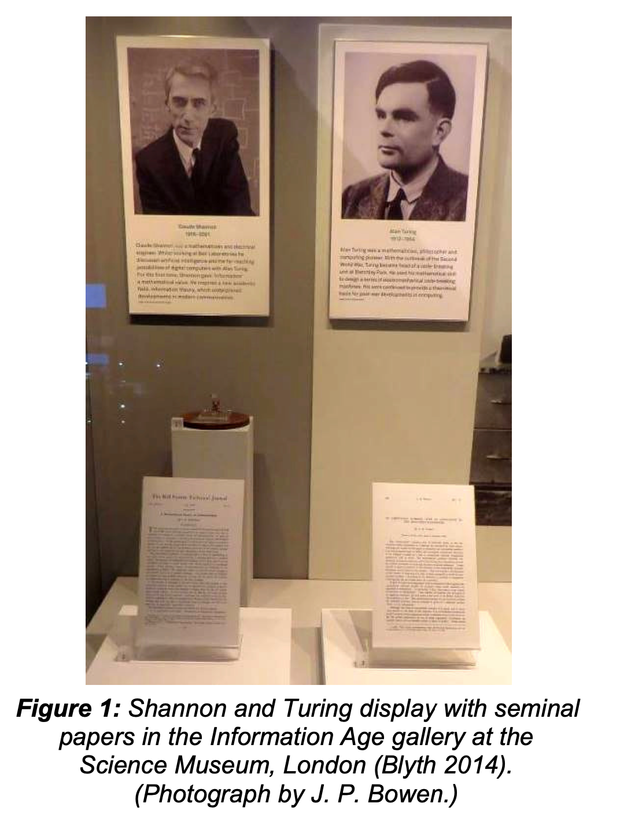
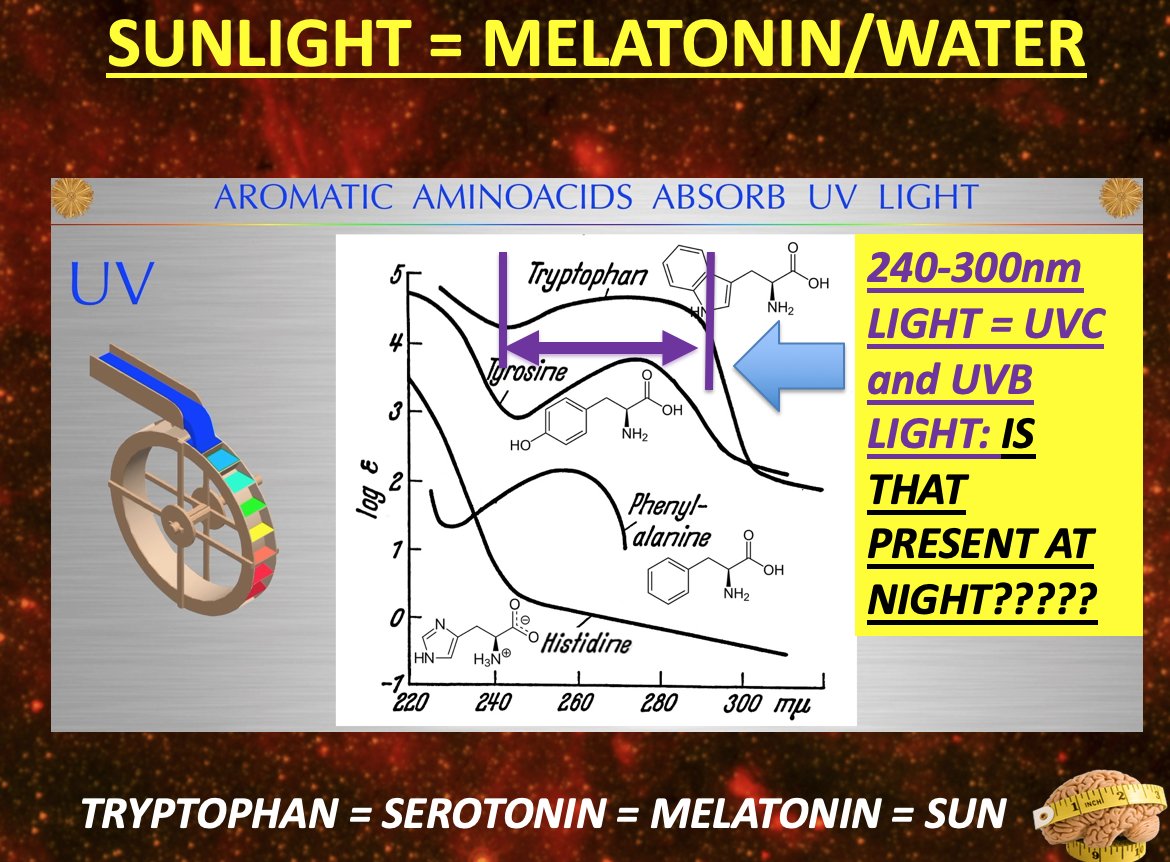
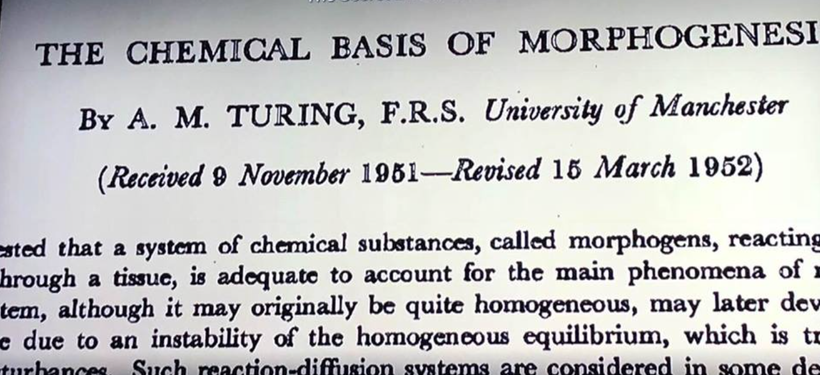

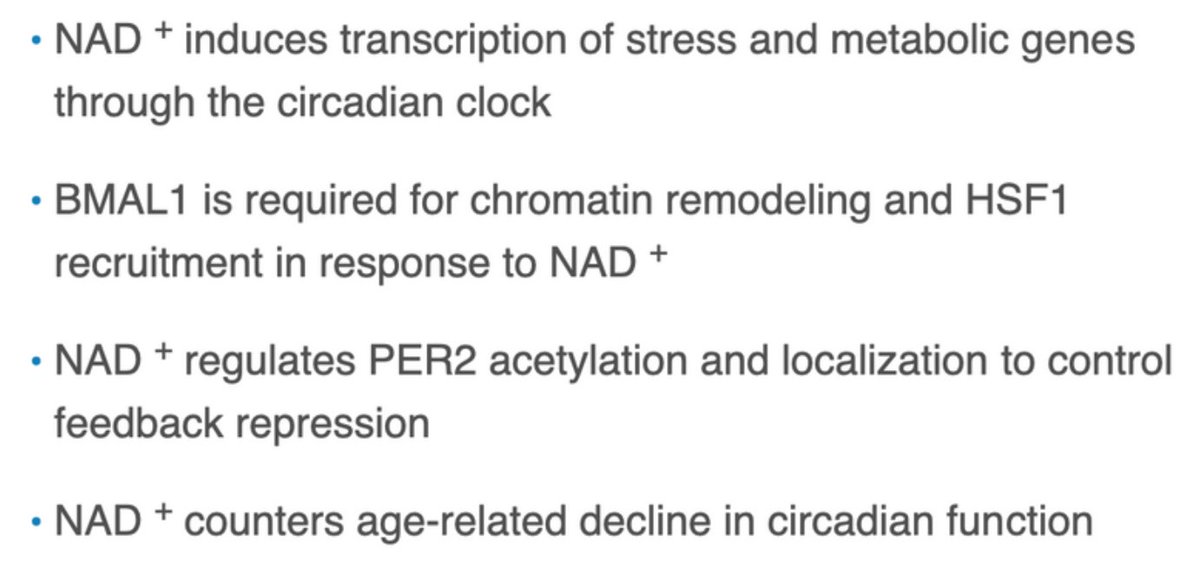
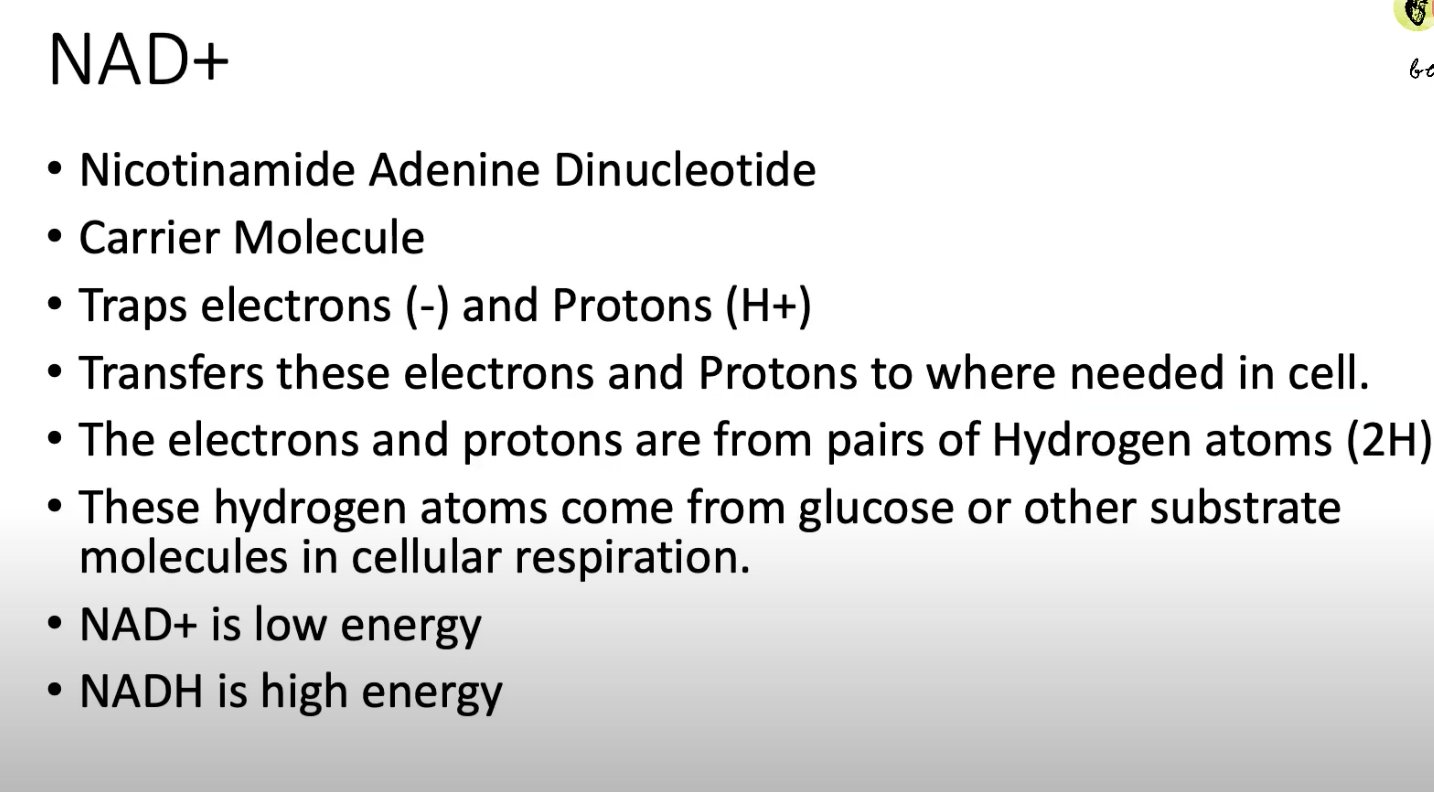
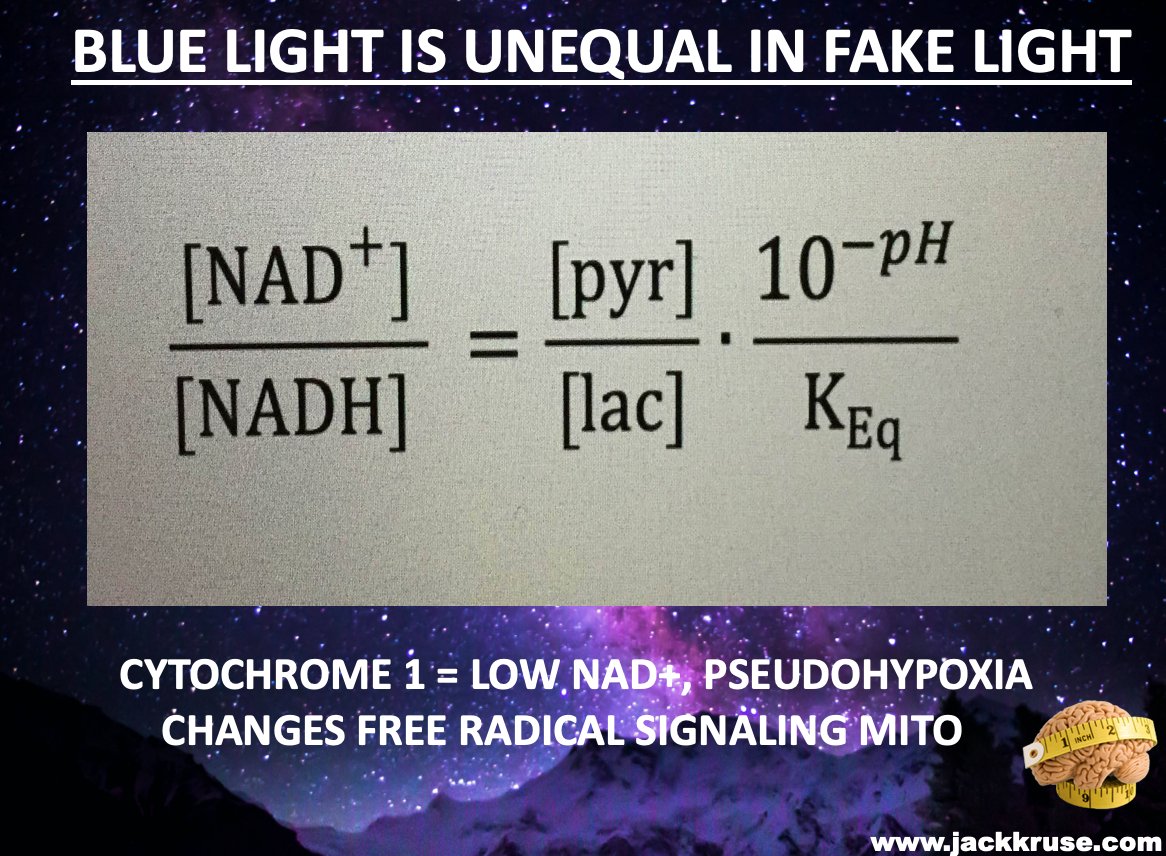
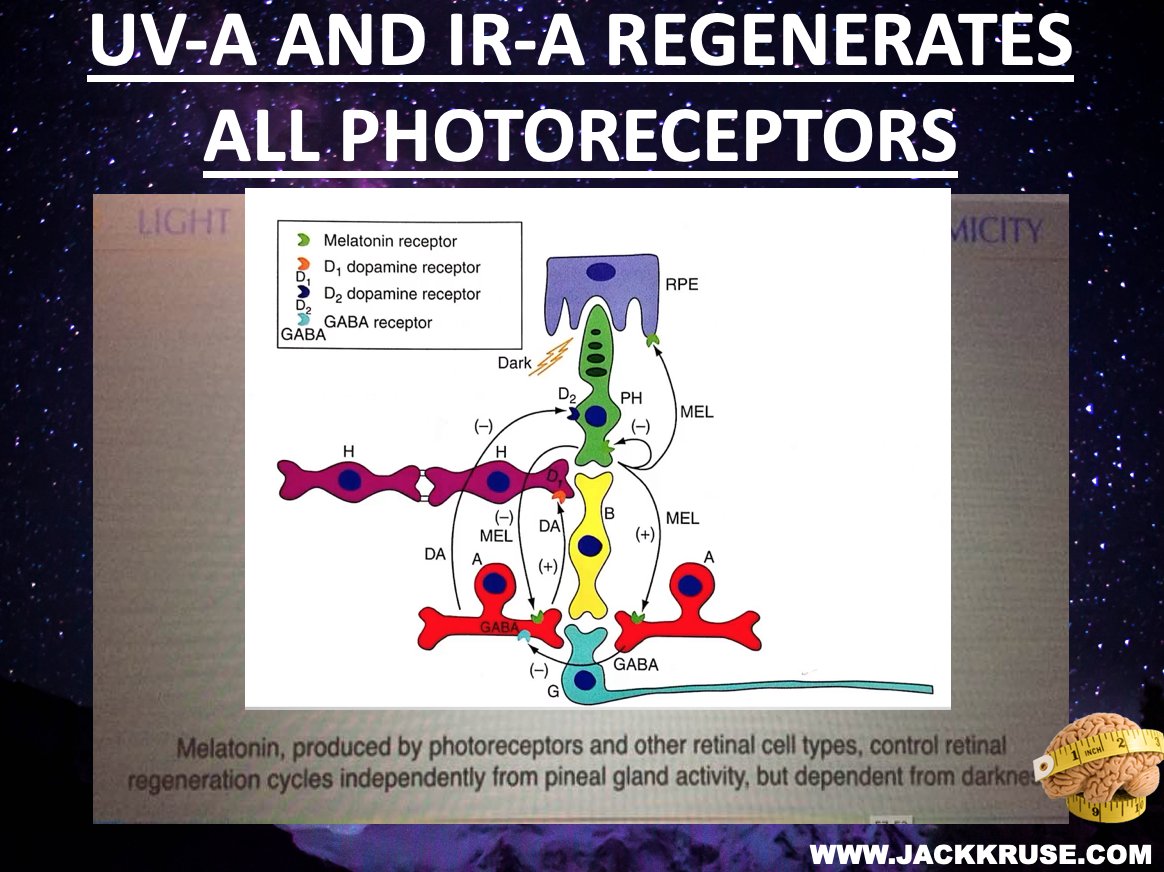
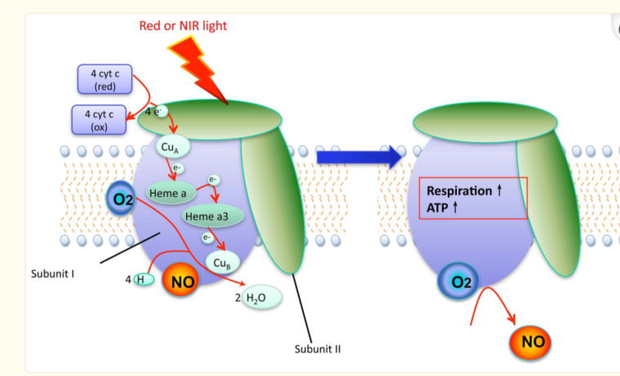
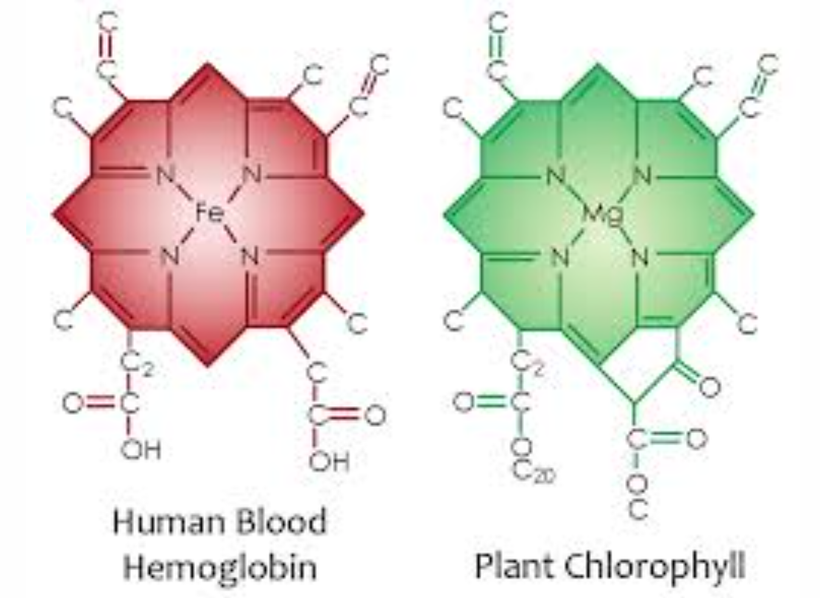


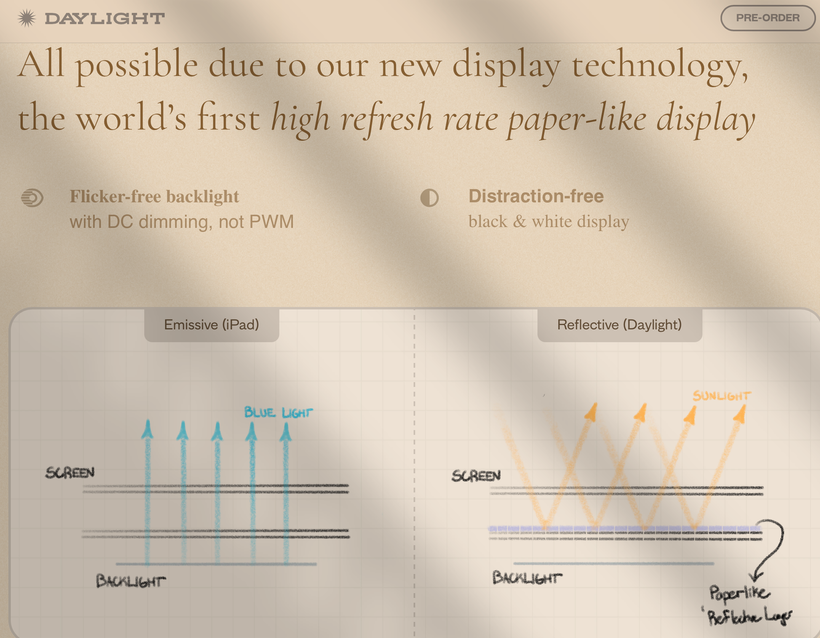
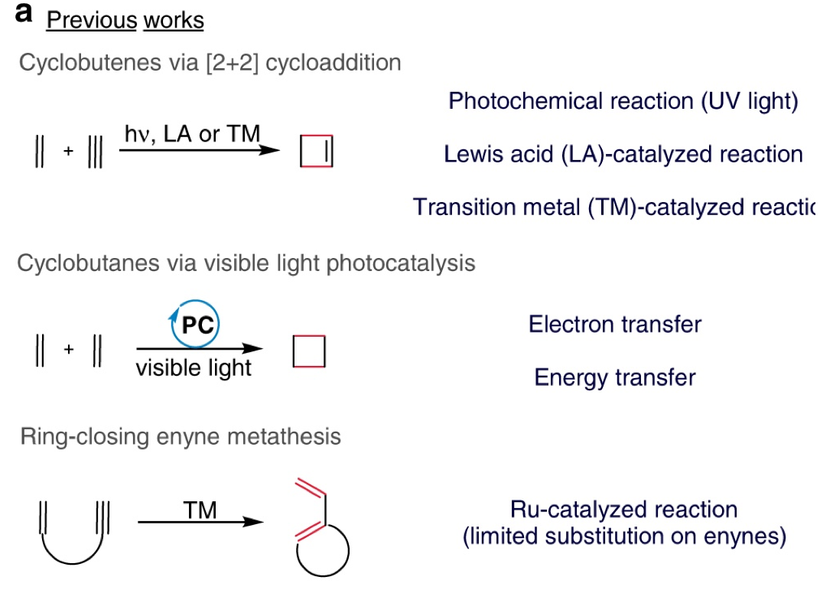
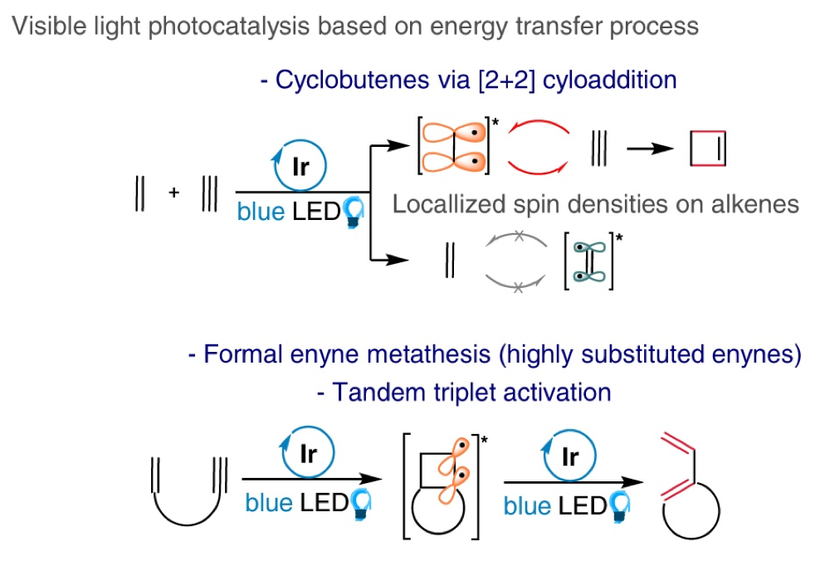

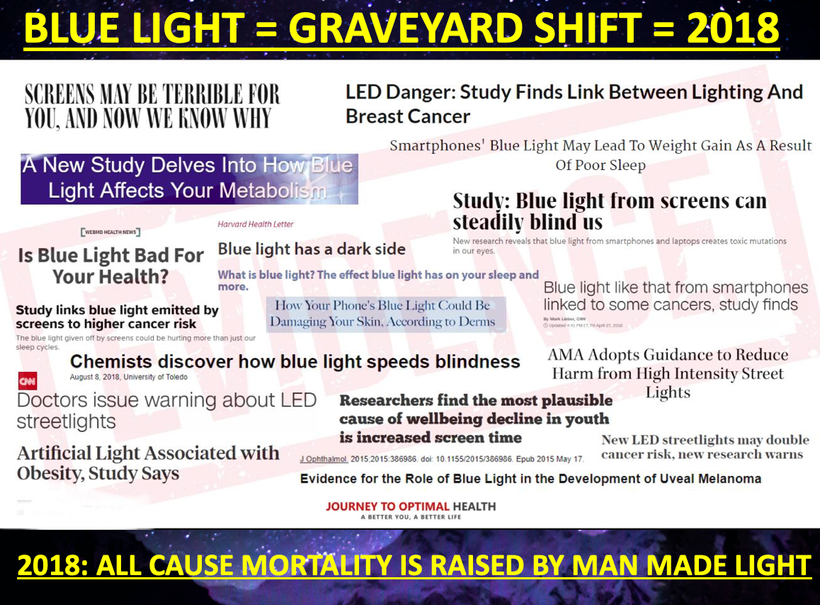









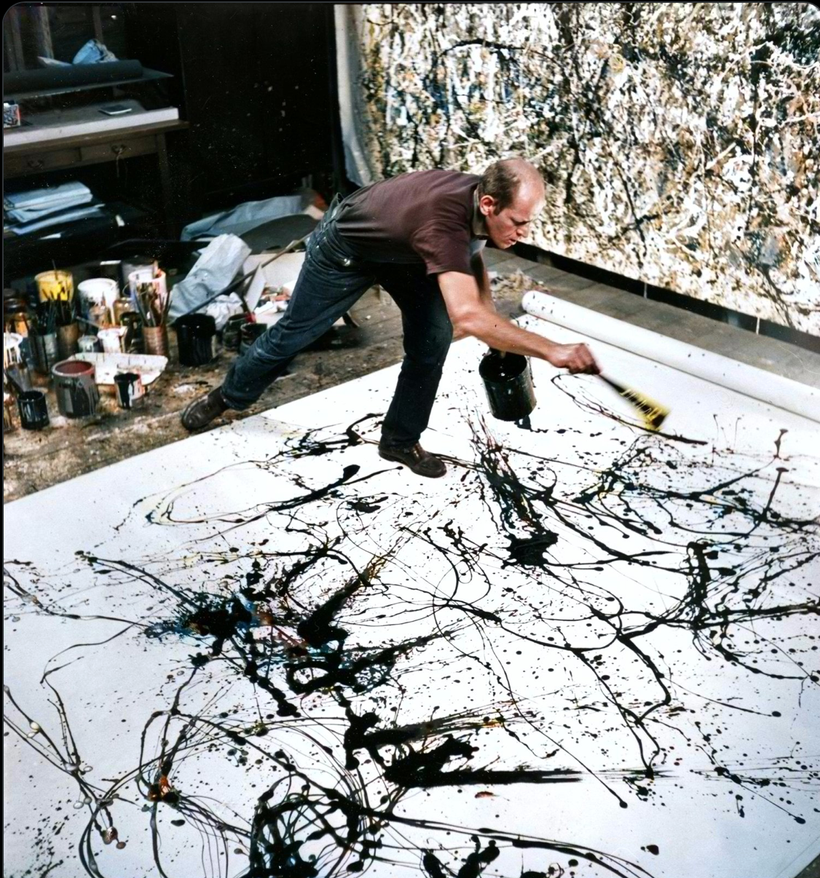

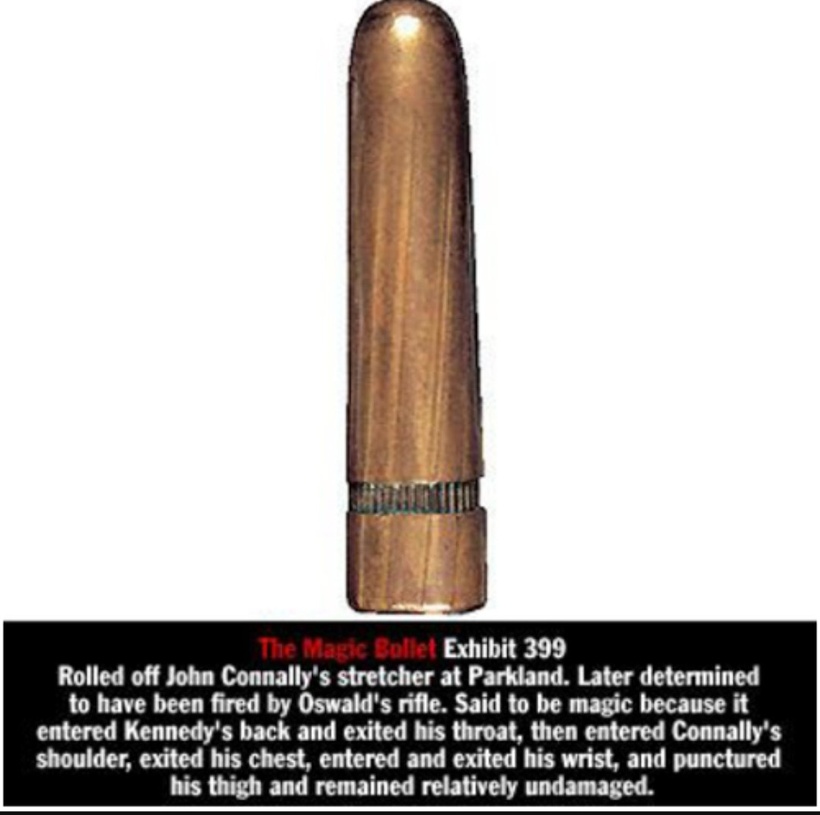

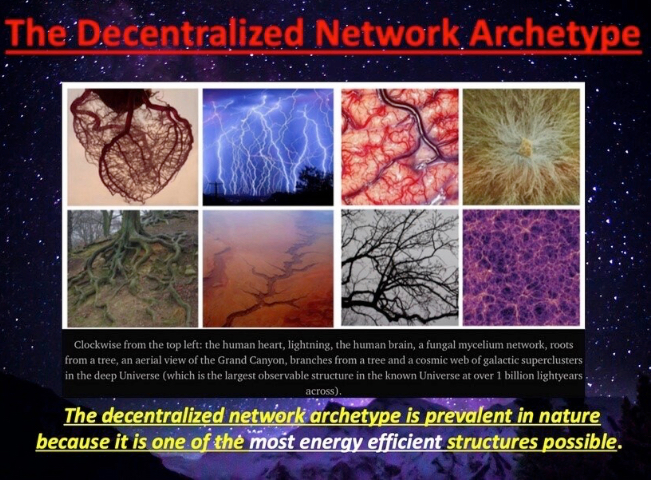

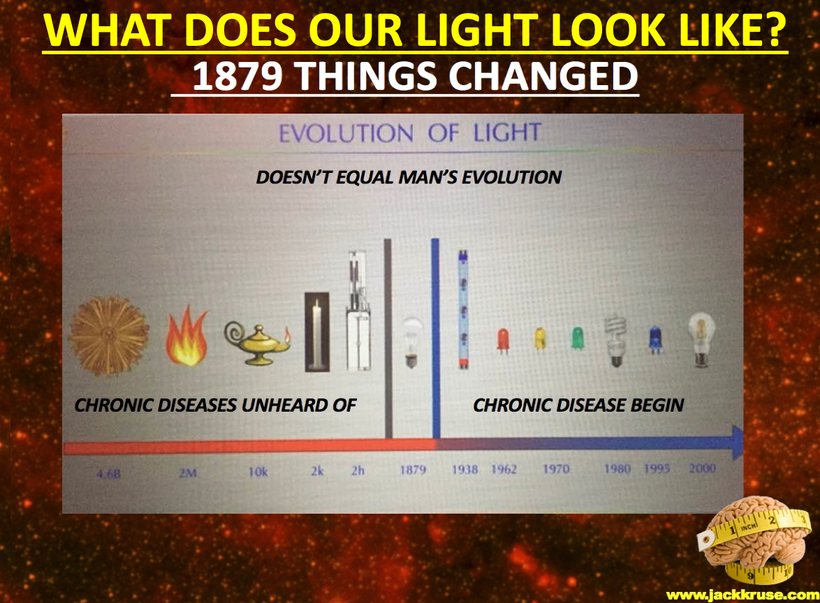
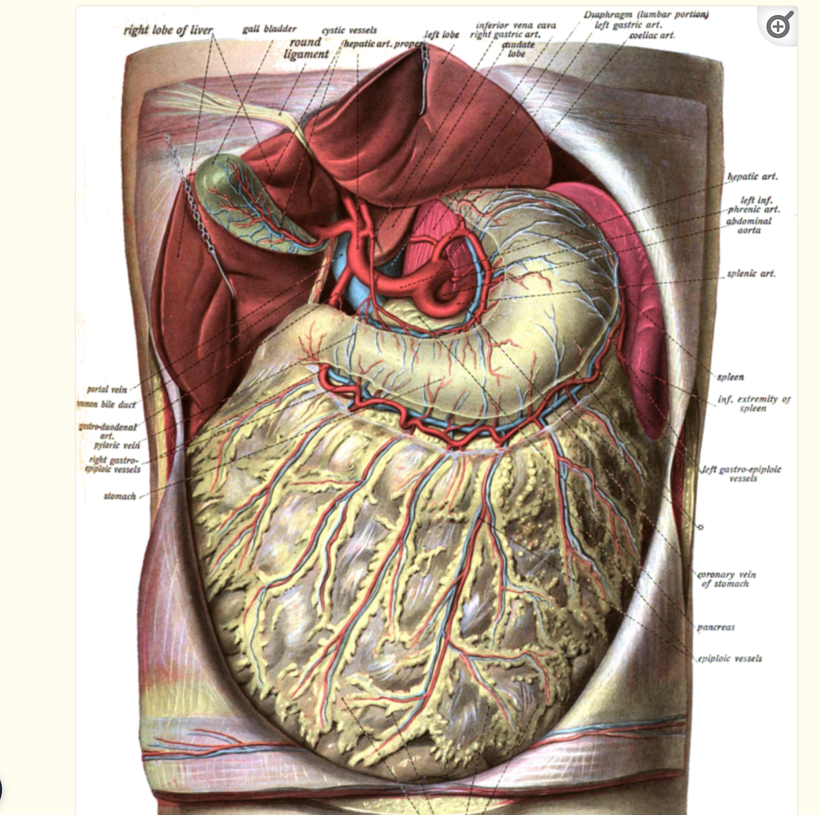
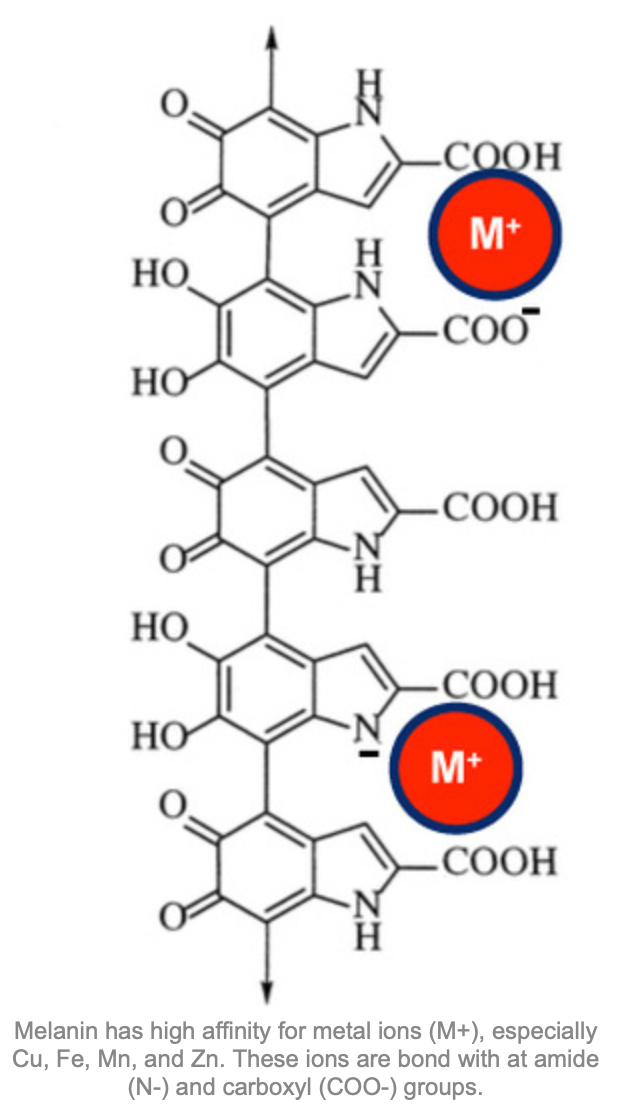
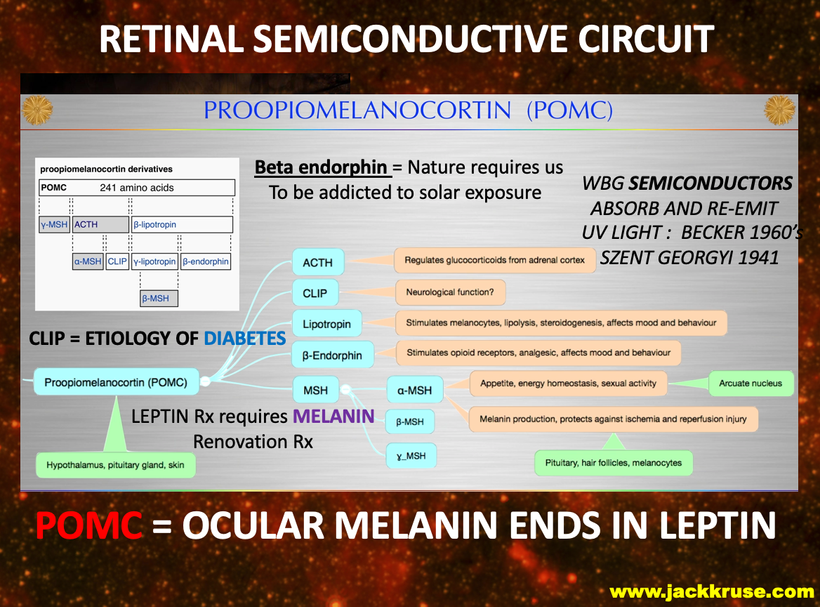
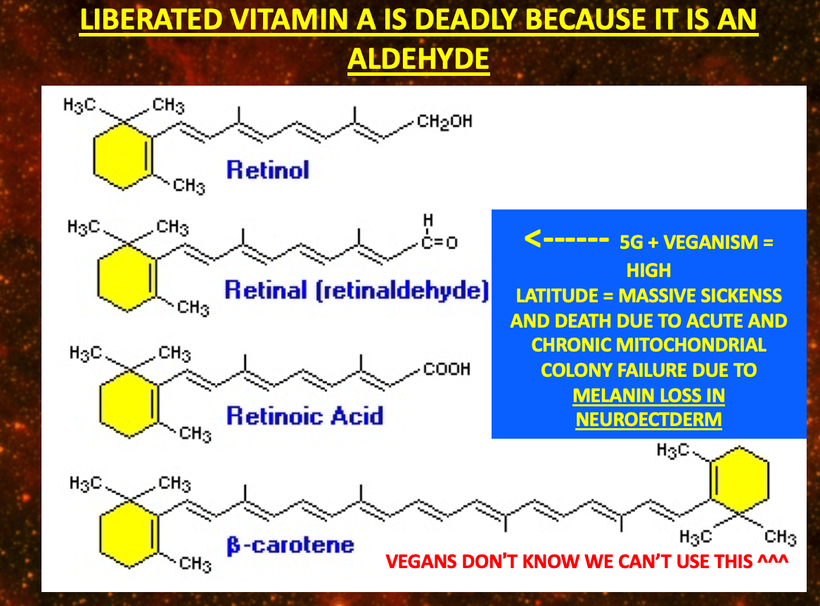
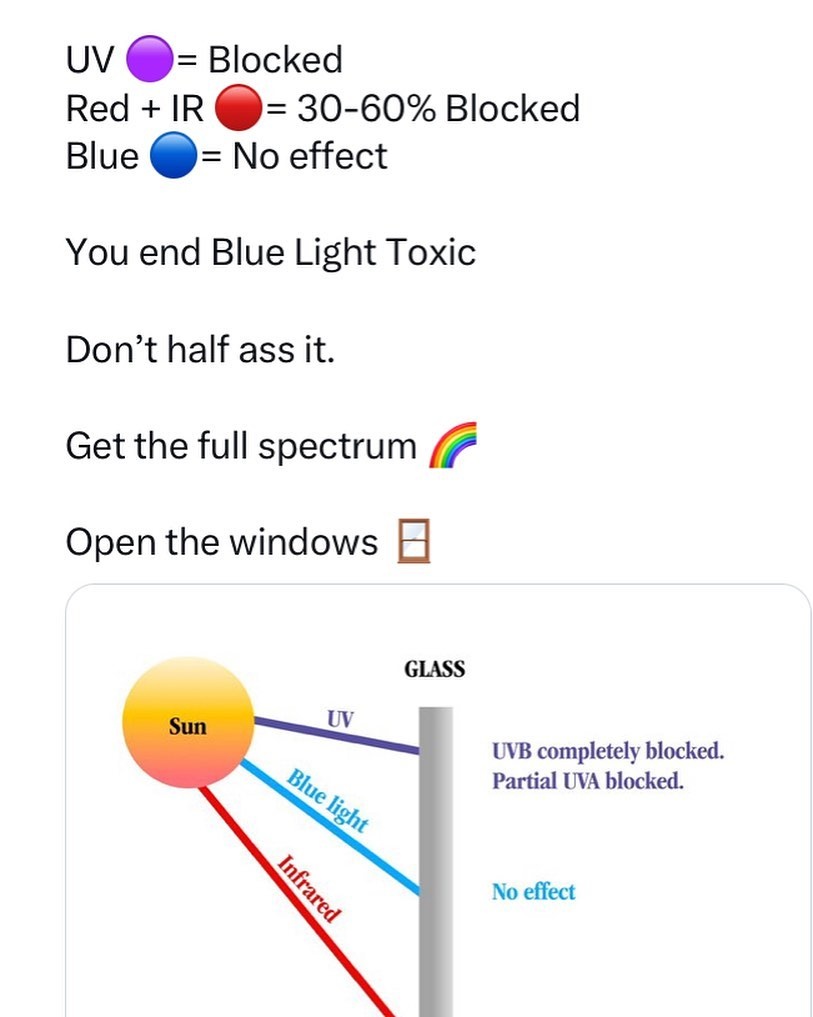



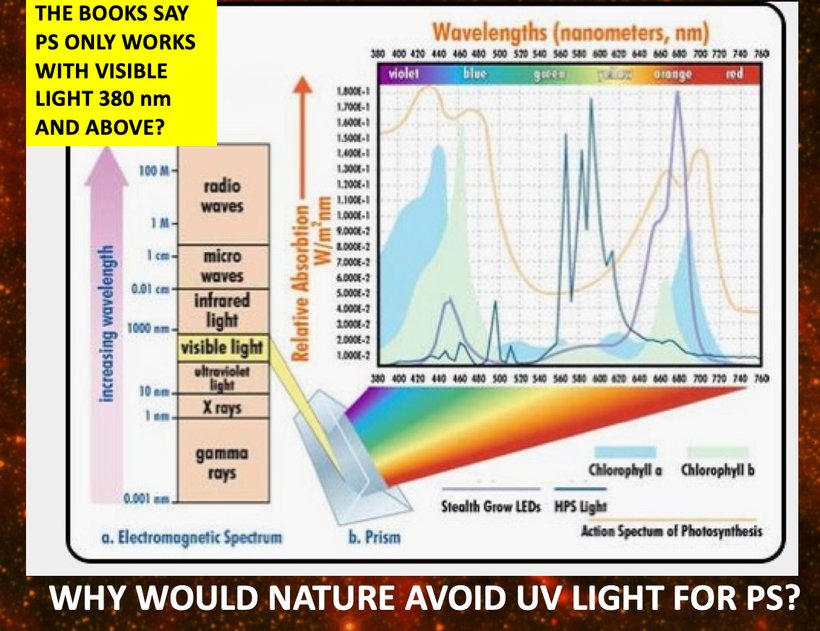
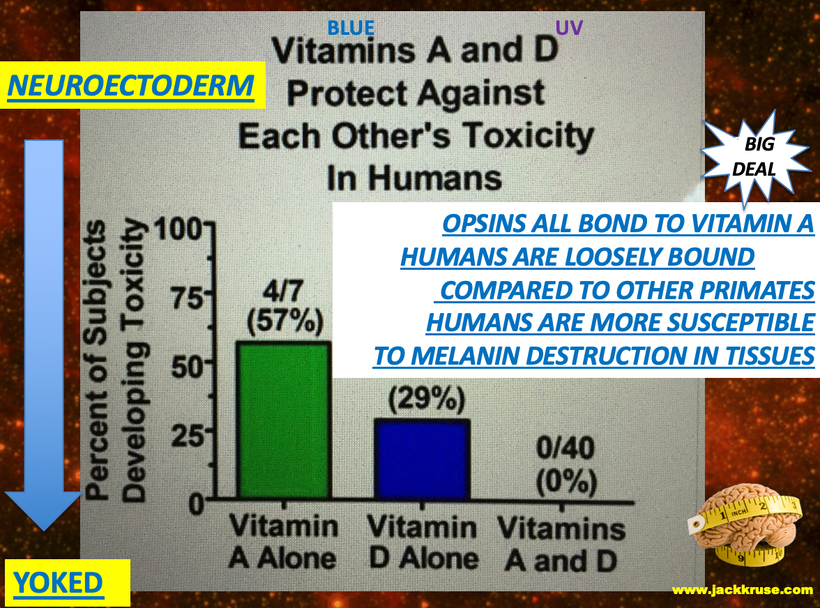
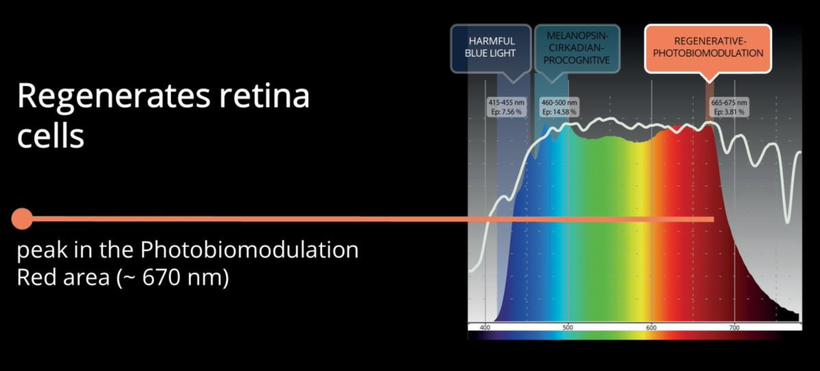
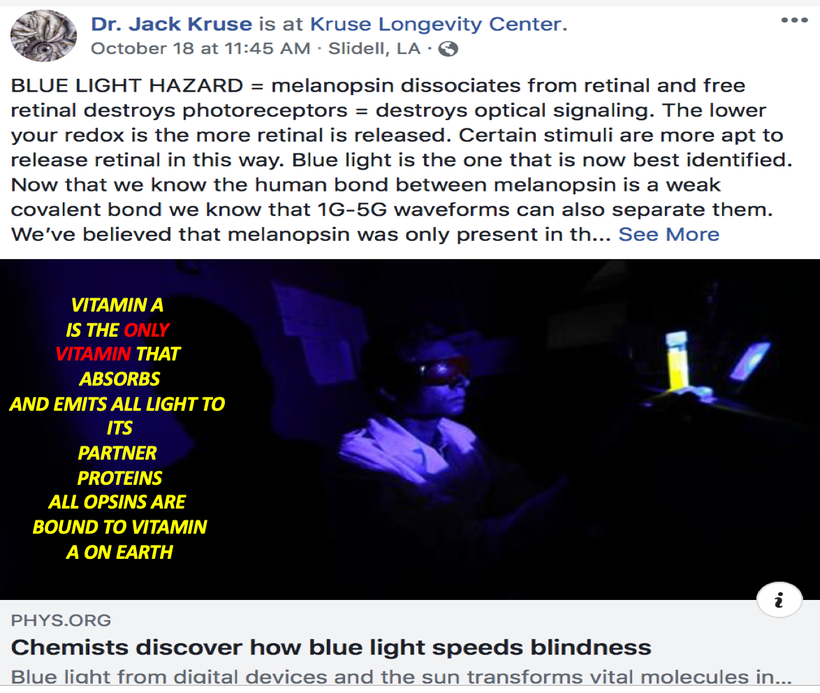
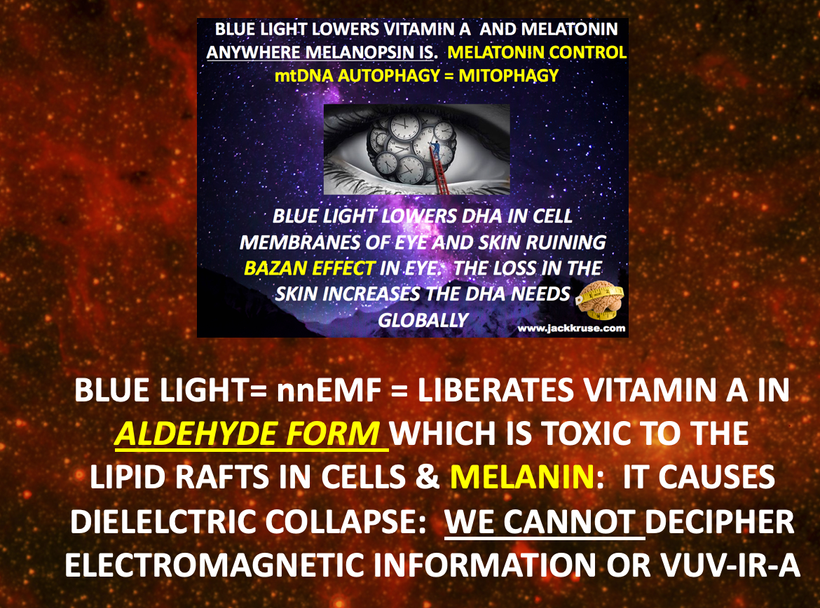
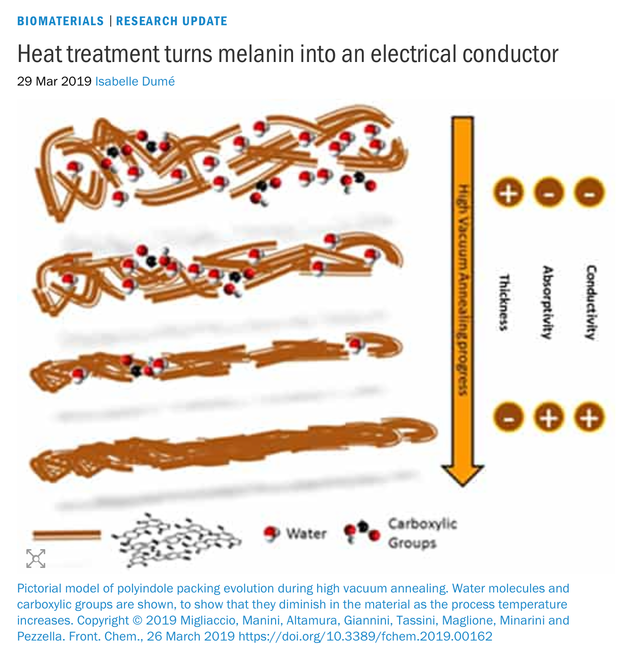
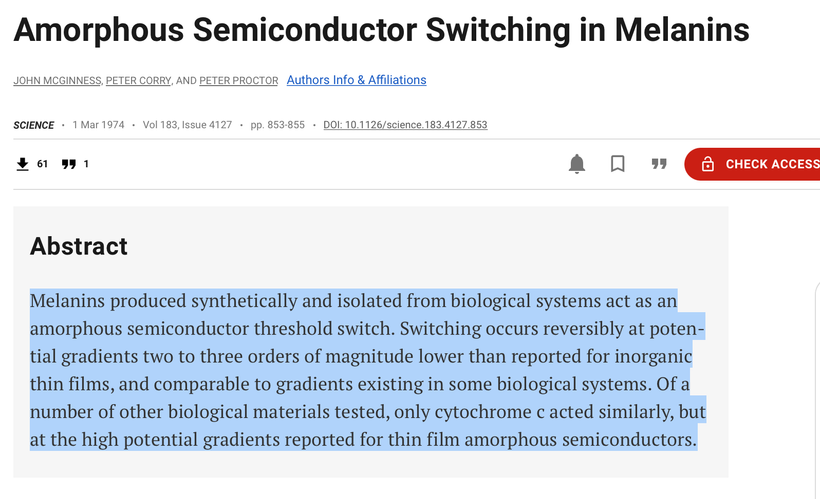
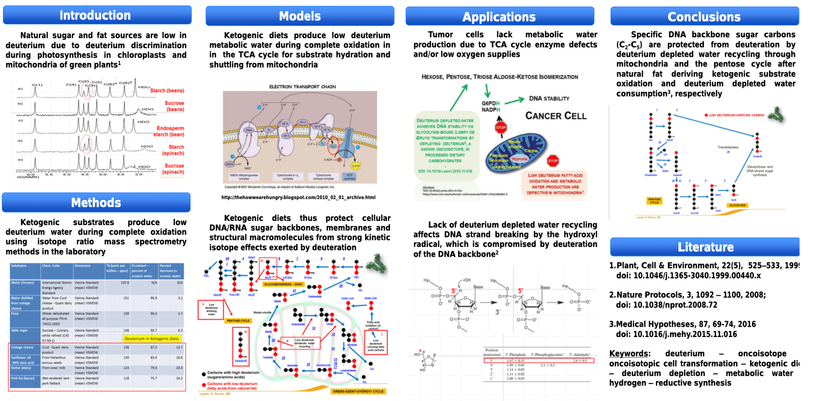
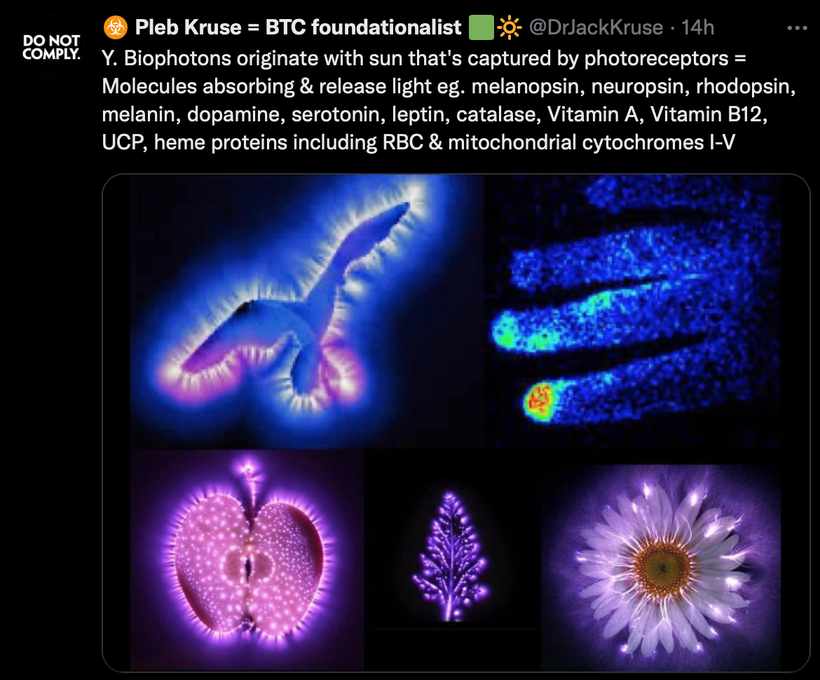
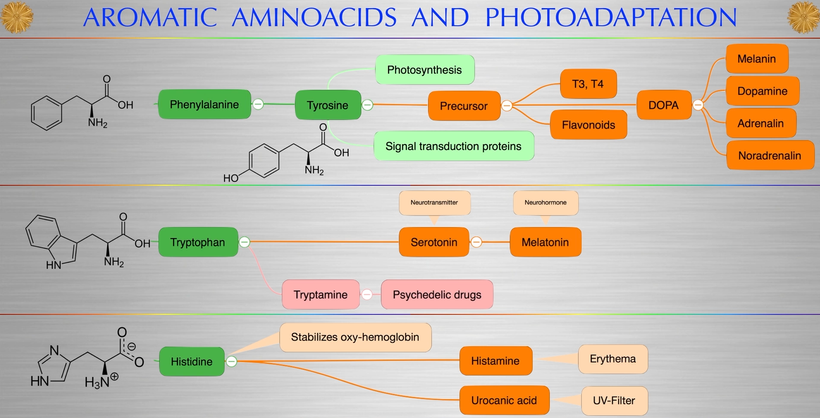

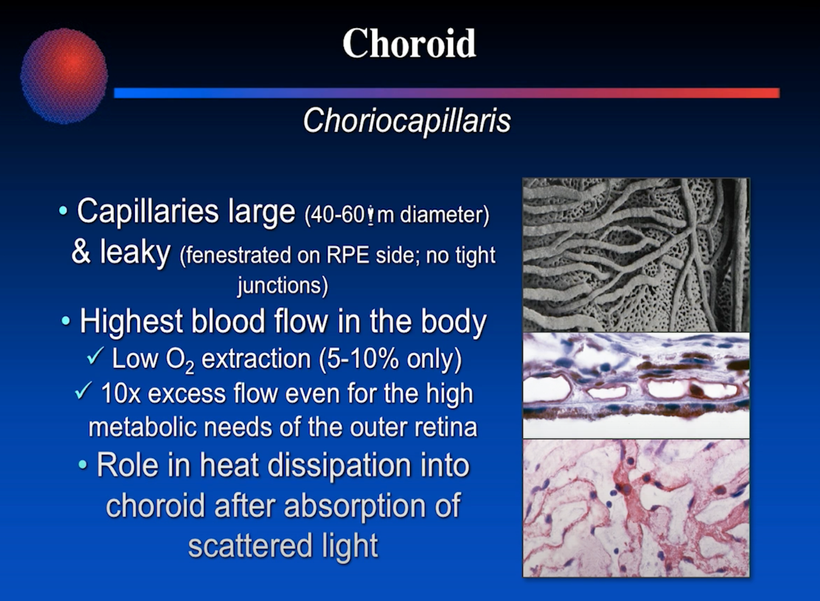
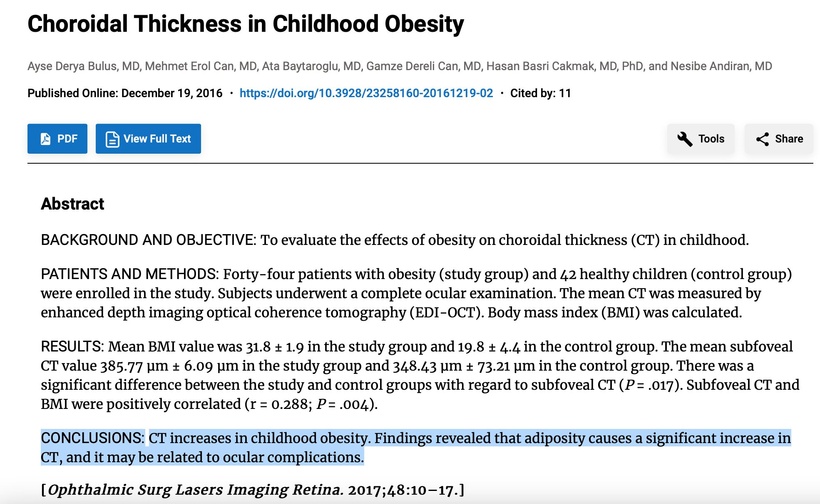
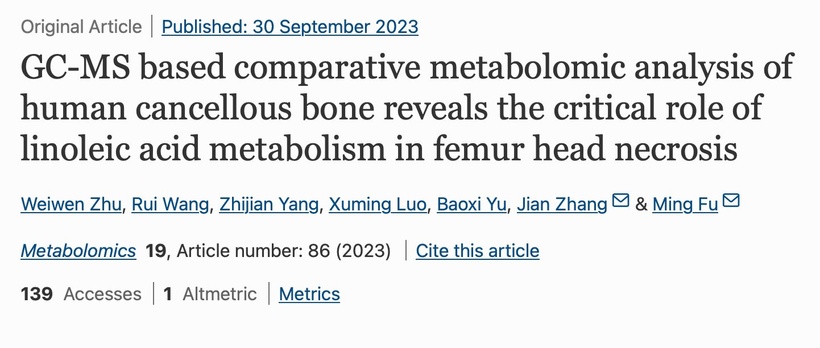
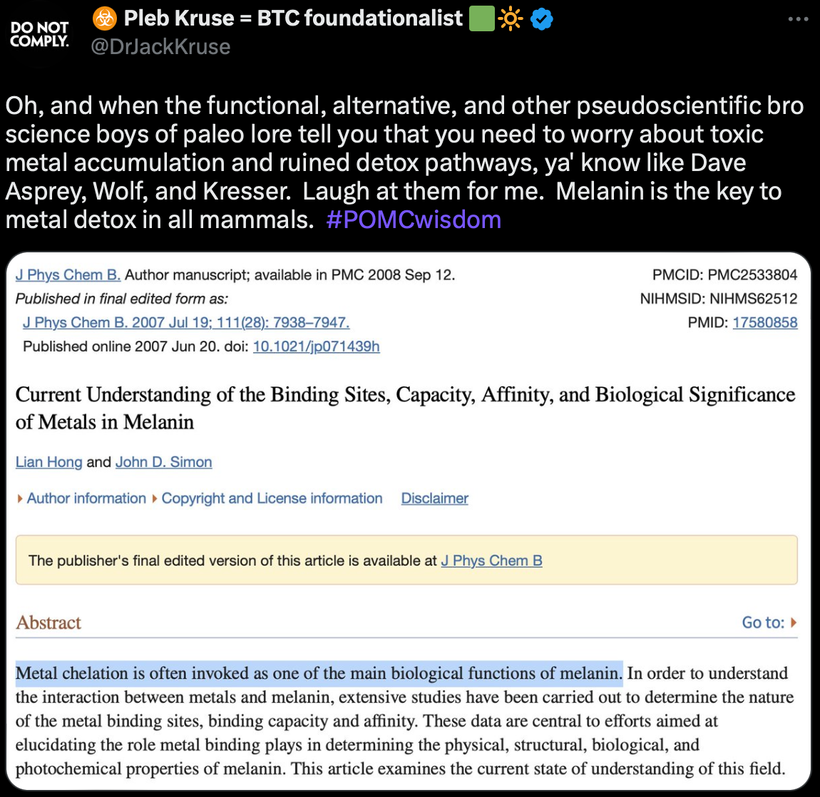



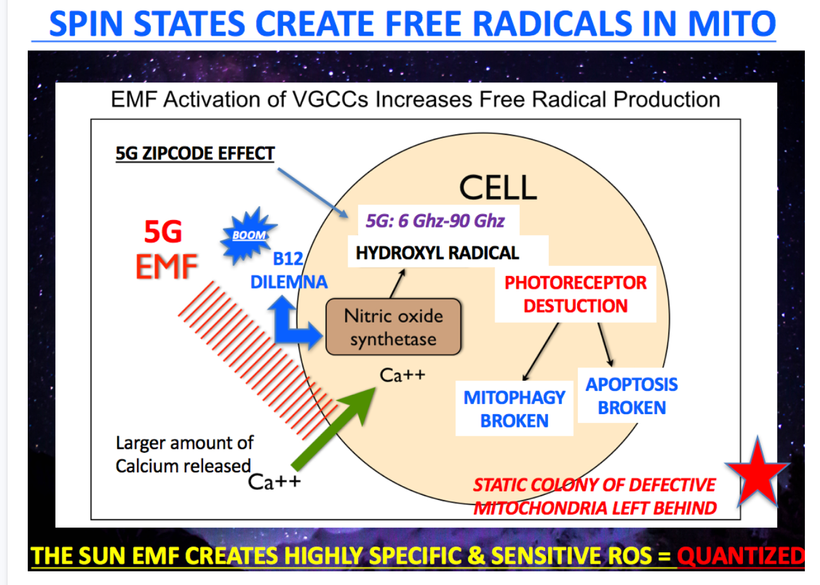
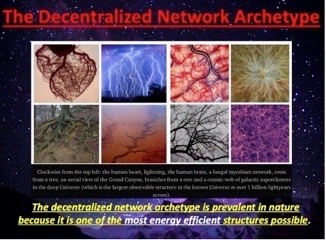
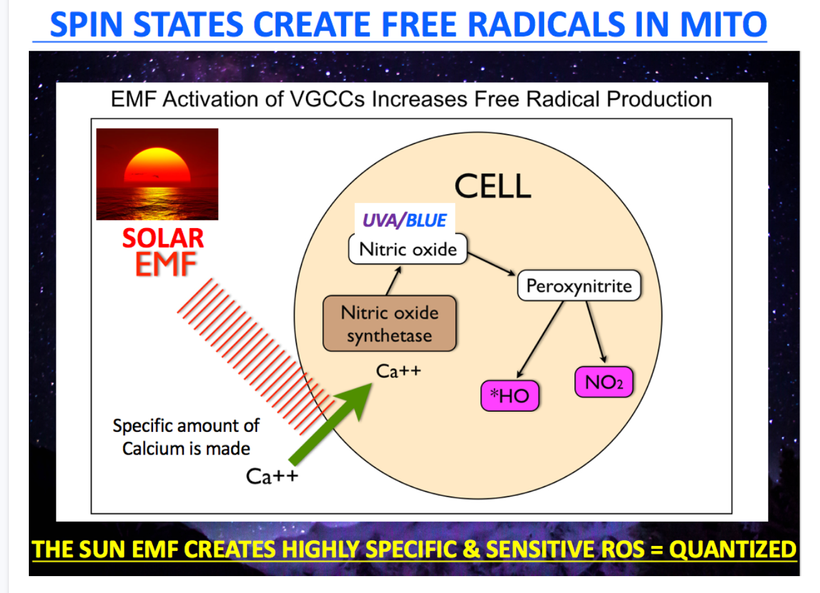

{kind=link}